When researchers and medical professionals investigate novel therapeutic peptides, understanding the complete safety profile becomes paramount. Mounjaro (Tirzepatide) Side Effects: What to Expect represents a critical area of inquiry as this dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist gains prominence in metabolic research. While tirzepatide demonstrates remarkable efficacy in clinical studies for glycaemic control and weight management, comprehensive knowledge of its adverse event profile ensures informed decision-making in research protocols and clinical applications.
The emergence of tirzepatide as a research compound has generated substantial interest within the scientific community, particularly regarding its tolerability and safety characteristics. This comprehensive guide examines Mounjaro (Tirzepatide) Side Effects: What to Expect across multiple dimensions—from common gastrointestinal manifestations to rare but serious adverse events—providing researchers, clinicians, and informed stakeholders with evidence-based insights into this peptide’s complete safety landscape.
Key Takeaways
- Gastrointestinal effects (nausea, vomiting, diarrhea) represent the most common side effects, typically occurring in 30-40% of subjects and often diminishing with continued exposure
- Dose-dependent patterns emerge clearly, with higher tirzepatide doses correlating with increased adverse event frequency and severity
- Temporal resolution characterizes most side effects, with peak incidence during initial weeks and dose escalation periods
- Serious adverse events remain relatively rare but include pancreatitis risk, thyroid concerns, and hypoglycaemia when combined with certain medications
- Proactive management strategies can significantly mitigate side effect burden and improve tolerability profiles in research and clinical settings
Understanding Tirzepatide’s Mechanism and Side Effect Origins

Tirzepatide’s unique pharmacological profile as a dual GIP/GLP-1 receptor agonist directly influences its side effect profile. Unlike single-target peptides, this compound engages two distinct incretin pathways simultaneously, producing enhanced metabolic effects but also contributing to its characteristic adverse event pattern[1].
The Incretin Connection
The GLP-1 receptor activation component of tirzepatide produces several physiological effects that underlie common side effects:
- Delayed gastric emptying: Slows food transit through the digestive system, contributing to feelings of fullness but also nausea
- Central nervous system effects: Acts on brainstem areas controlling satiety and nausea responses
- Intestinal motility changes: Alters normal digestive rhythm and fluid secretion patterns
The GIP receptor activation adds complementary metabolic benefits while potentially modulating the intensity of GLP-1-mediated effects. Research suggests the dual mechanism may actually improve tolerability compared to GLP-1-only agonists in some parameters, though individual responses vary considerably[2].
Peptide Purity and Research Considerations
For researchers sourcing tirzepatide for laboratory investigations, peptide quality directly impacts experimental outcomes and safety profiles. High-purity research-grade peptides ensure consistent results and minimize confounding variables introduced by impurities or degradation products. Institutions conducting tirzepatide research should prioritize suppliers offering comprehensive certificates of analysis and proper storage protocols.
Common Mounjaro (Tirzepatide) Side Effects: What to Expect in Clinical Practice
Gastrointestinal Effects: The Predominant Category
Gastrointestinal adverse events dominate the tirzepatide side effect profile, representing the most frequently reported category across clinical trials and real-world evidence.
Nausea emerges as the single most common side effect, with incidence rates varying by dose:
| Tirzepatide Dose | Nausea Incidence | Severity Profile |
|---|---|---|
| 5 mg | 12-17% | Predominantly mild |
| 10 mg | 18-22% | Mild to moderate |
| 15 mg | 21-25% | Moderate predominant |
Diarrhea represents the second most common gastrointestinal effect, occurring in approximately 13-16% of subjects across dosing ranges. This typically manifests as:
- Increased stool frequency (3-5 bowel movements daily)
- Loose or watery consistency
- Occasional urgency
- Usually self-limiting within 2-4 weeks
Vomiting affects 5-9% of subjects, generally occurring in those experiencing more severe nausea. This adverse event shows strong correlation with:
- Rapid dose escalation
- Large meal consumption
- High-fat dietary intake
- Individual susceptibility factors
Constipation paradoxically affects 6-8% of subjects, demonstrating tirzepatide’s variable effects on intestinal motility. This appears more common in:
- Subjects with pre-existing slow transit
- Those with inadequate hydration
- Individuals with low dietary fiber intake
Appetite and Eating-Related Effects
Beyond direct gastrointestinal symptoms, tirzepatide produces appetite-related effects that subjects should anticipate:
- Reduced appetite: Nearly universal, representing the intended therapeutic mechanism
- Early satiety: Feeling full after small meal portions
- Food aversion: Temporary disinterest in previously enjoyed foods
- Altered taste: Metallic or changed taste perception in 3-5% of subjects
These effects, while contributing to weight loss efficacy, may require dietary strategy adjustments. Researchers investigating peptide-based metabolic interventions should document these subjective effects systematically as they significantly impact subject compliance and quality of life metrics.
Injection Site Reactions
Local reactions at subcutaneous injection sites occur in approximately 2-4% of subjects:
- Erythema (redness): 1-2 cm diameter, resolving within 24-48 hours
- Mild pain or tenderness: Transient, typically <30 minutes duration
- Induration (firmness): Occasional, resolving within days
- Bruising: Related to injection technique and individual factors
Proper injection technique and site rotation minimize these reactions. Research protocols should include standardized injection training to reduce technique-related adverse events.
Dose-Dependent Side Effects and Escalation Strategies
The Dose-Response Relationship
Clinical trial data clearly demonstrates dose-dependent increases in adverse event frequency and severity. Understanding this relationship proves essential for Mounjaro (Tirzepatide) Side Effects: What to Expect across different dosing protocols.
Comparative Incidence by Dose:
- 2.5 mg (starting dose): Lowest adverse event rate, primarily mild nausea (8-12%)
- 5 mg: Moderate increase in GI effects (15-20% combined)
- 7.5 mg: Notable escalation in nausea and diarrhea (22-28%)
- 10 mg: Higher incidence across all GI categories (28-35%)
- 12.5 mg: Further increases, particularly vomiting (32-40%)
- 15 mg (maximum approved): Highest adverse event rates (35-45% GI effects)
Optimal Escalation Protocols
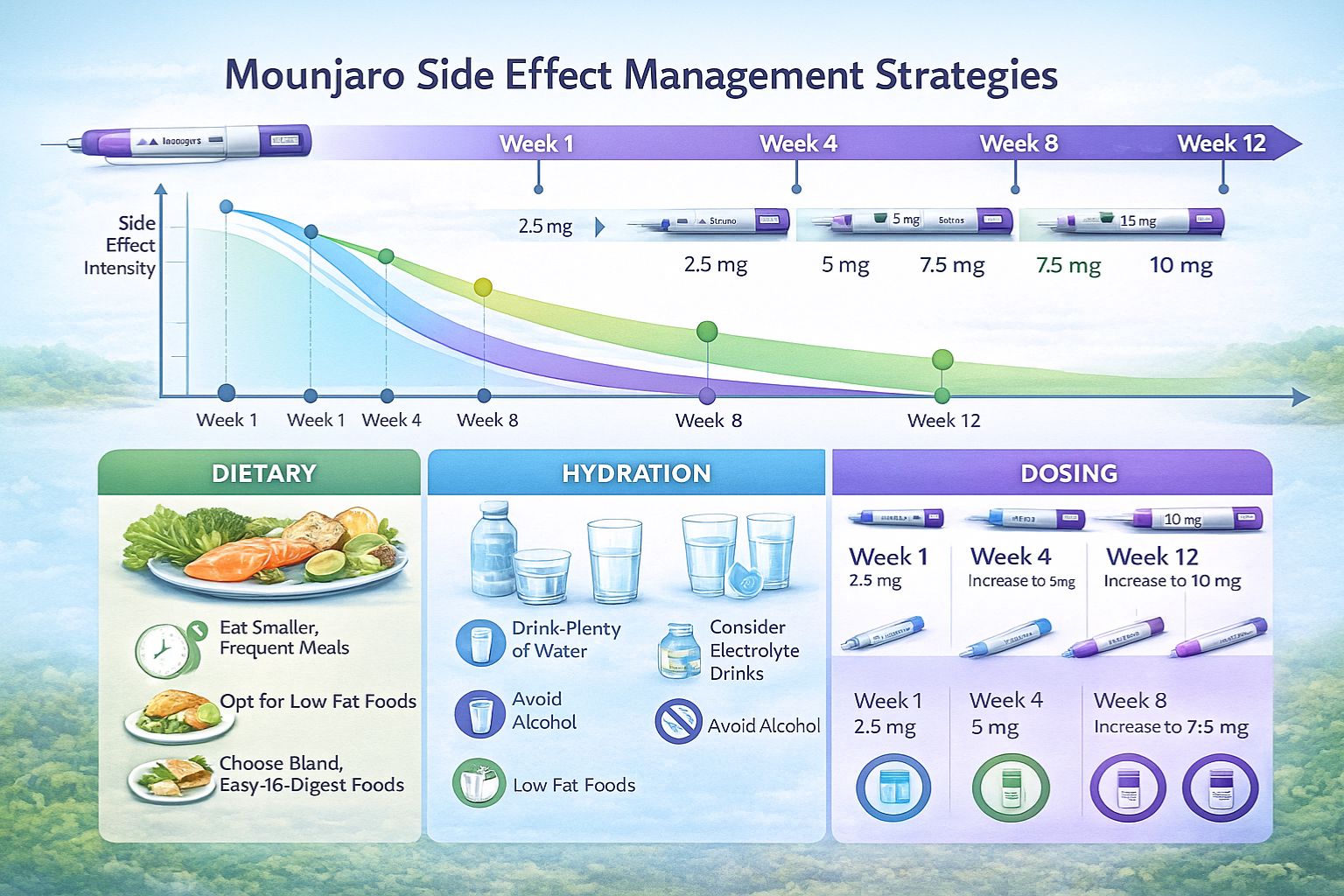
Evidence-based dose escalation significantly impacts tolerability. The standard protocol involves:
- Week 1-4: 2.5 mg weekly
- Week 5-8: 5 mg weekly
- Week 9-12: 7.5 mg weekly (if needed)
- Week 13-16: 10 mg weekly (if needed)
- Week 17+: 12.5-15 mg weekly (if needed)
This gradual escalation allows physiological adaptation and minimizes adverse event severity. Researchers designing tirzepatide protocols should incorporate adequate escalation periods and document tolerance at each transition point[3].
Individual Variation and Predictive Factors
Substantial inter-individual variation characterizes tirzepatide tolerability. Factors associated with higher side effect burden include:
- Female sex: Consistently higher nausea and vomiting rates
- Younger age: Greater GI sensitivity in subjects <40 years
- History of motion sickness: Strong predictor of nausea susceptibility
- Gastroparesis or dyspepsia history: Significantly increased risk
- Concurrent medications: Particularly those affecting GI motility
Serious and Rare Mounjaro (Tirzepatide) Side Effects: What to Expect
Pancreatitis Risk
Acute pancreatitis represents the most concerning serious adverse event associated with GLP-1 receptor agonists, including tirzepatide. While rare (estimated 0.2-0.5% incidence), this potentially severe condition requires immediate recognition[4].
Warning Signs:
- Severe, persistent abdominal pain radiating to the back
- Nausea and vomiting unresponsive to standard management
- Fever and elevated heart rate
- Abdominal tenderness on examination
Risk Factors:
- History of pancreatitis
- Gallstone disease
- Hypertriglyceridemia (>500 mg/dL)
- Excessive alcohol consumption
- Certain genetic predispositions
Research protocols should exclude subjects with pancreatitis history and establish clear discontinuation criteria if symptoms develop.
Thyroid C-Cell Concerns
Preclinical rodent studies demonstrated thyroid C-cell tumors with GLP-1 receptor agonists, leading to boxed warnings. However, relevance to humans remains uncertain:
- Rodent models: Dose-dependent C-cell hyperplasia and medullary thyroid carcinoma
- Human relevance: Uncertain due to species differences in GLP-1 receptor distribution
- Clinical surveillance: No confirmed cases causally linked to tirzepatide
- Contraindication: Personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
Researchers should screen subjects for thyroid cancer history and MEN 2 before protocol enrollment.
Hypoglycaemia Risk
Tirzepatide monotherapy rarely causes hypoglycaemia due to its glucose-dependent mechanism. However, risk increases substantially when combined with:
- Insulin: Requires dose reduction of 20-30% when initiating tirzepatide
- Sulfonylureas: Similarly requires preemptive dose adjustment
- Meglitinides: Moderate risk, may require modification
Hypoglycaemia symptoms to monitor:
- Tremor, palpitations, sweating
- Confusion, difficulty concentrating
- Hunger, irritability
- Dizziness, weakness
Research protocols combining tirzepatide with other glucose-lowering agents should implement frequent glucose monitoring and predetermined dose adjustment algorithms.
Acute Kidney Injury
Severe gastrointestinal side effects may precipitate dehydration-related acute kidney injury, particularly in vulnerable populations:
- Mechanism: Volume depletion from vomiting/diarrhea
- Risk factors: Pre-existing chronic kidney disease, diuretic use, advanced age
- Incidence: Rare (<0.5%) but potentially serious
- Prevention: Adequate hydration counseling, monitoring of renal function
Gallbladder and Biliary Disease
Rapid weight loss associated with tirzepatide may increase cholelithiasis (gallstone) risk:
- Mechanism: Altered bile composition and gallbladder motility during rapid weight reduction
- Incidence: Approximately 1.5-2.5% across clinical trials
- Presentation: Right upper quadrant pain, nausea, possible jaundice
- Management: Ultrasound evaluation, possible cholecystectomy
Subjects experiencing characteristic biliary pain should undergo prompt evaluation.
Allergic and Hypersensitivity Reactions
Serious allergic reactions remain rare but documented:
- Anaphylaxis: Extremely rare (<0.1%) but potentially life-threatening
- Angioedema: Swelling of face, lips, tongue, throat
- Urticaria: Widespread hives
- Respiratory symptoms: Wheezing, difficulty breathing
Research facilities should maintain emergency protocols and epinephrine availability when administering peptide compounds. For laboratories seeking diverse peptide research options, proper safety protocols remain paramount across all compounds.
Temporal Patterns: When Mounjaro (Tirzepatide) Side Effects Occur
Initial Exposure Period (Weeks 1-4)
The first month of tirzepatide exposure typically represents the highest-risk period for adverse events:
Week 1-2:
- Peak nausea incidence (often 2-5 days post-first injection)
- Appetite suppression most pronounced
- Fatigue and mild headache common
- Injection site reactions if occurring
Week 3-4:
- Gradual symptom improvement in most subjects
- Physiological adaptation beginning
- Continued appetite effects
- Stabilization of GI symptoms
Dose Escalation Periods
Each dose increase may temporarily reactivate side effects:
- Pattern: Symptoms often recur at 50-70% of initial intensity
- Duration: Typically shorter than initial exposure (3-7 days vs. 7-14 days)
- Adaptation: Progressive improvement in tolerance with each escalation
- Individual variation: Some subjects experience minimal recurrence, others more pronounced
Long-Term Patterns (Months 3-12+)
Extended tirzepatide exposure generally shows favorable tolerability trends:
- GI effects: Substantial reduction, with 60-75% of subjects reporting resolution
- Persistent nausea: Affects 5-10% of long-term users
- Appetite suppression: Continues but often less intense
- New-onset effects: Uncommon after 3-month stabilization period
Research protocols extending beyond 6 months should continue systematic adverse event monitoring, as late-onset effects occasionally emerge.
Management Strategies for Mounjaro (Tirzepatide) Side Effects
Dietary Modifications
Strategic dietary adjustments significantly impact tolerability:
For Nausea:
- Small, frequent meals (5-6 daily vs. 3 large meals)
- Bland, low-fat options during symptomatic periods
- Ginger supplementation (250-500 mg, 2-3 times daily)
- Avoiding strong odors and trigger foods
- Cold or room-temperature foods better tolerated than hot
For Diarrhea:
- Increased soluble fiber (psyllium, oats)
- Probiotic supplementation
- Adequate electrolyte replacement
- Temporary reduction in fat intake
- BRAT diet during acute episodes (bananas, rice, applesauce, toast)
For Constipation:
- Increased water intake (2-3 liters daily)
- Insoluble fiber sources (vegetables, whole grains)
- Regular physical activity
- Magnesium supplementation (200-400 mg daily)
- Stool softeners if needed
Hydration Protocols
Maintaining adequate hydration proves critical for minimizing complications:
- Target intake: Minimum 2 liters daily, increased during GI symptoms
- Electrolyte balance: Consider electrolyte solutions during vomiting/diarrhea
- Monitoring: Urine color assessment (pale yellow indicates adequate hydration)
- Timing: Consistent intake throughout day rather than large boluses
Pharmacological Interventions
When non-pharmacological approaches prove insufficient:
Anti-nausea medications:
- Ondansetron (4-8 mg as needed): Highly effective, minimal interactions
- Metoclopramide (10 mg before meals): Prokinetic effect beneficial
- Prochlorperazine (5-10 mg as needed): Alternative option
- Ginger supplements: Natural option with modest efficacy
Anti-diarrheal agents:
- Loperamide (2-4 mg as needed, maximum 16 mg daily): First-line option
- Bismuth subsalicylate: Additional anti-inflammatory benefit
- Diphenoxylate/atropine: Alternative for refractory cases
Caution: Chronic use of anti-motility agents not recommended; address underlying cause.
Dose Adjustment Strategies
When side effects prove intolerable despite management efforts:
- Temporary dose reduction: Return to previous tolerated dose for 2-4 additional weeks
- Slower escalation: Extend time at each dose level (6-8 weeks vs. 4 weeks)
- Alternative dosing: Some protocols explore every-10-day dosing for better tolerance
- Discontinuation: Consider if severe effects persist despite interventions
Research protocols should predefine dose modification criteria and discontinuation thresholds.
Special Populations and Considerations
Renal Impairment
Tirzepatide undergoes proteolytic degradation rather than renal elimination, but considerations include:
- Mild-moderate impairment (eGFR 30-89): No dose adjustment required
- Severe impairment (eGFR 15-29): Limited data; use with caution
- End-stage renal disease: Insufficient evidence; generally not recommended
- Dehydration risk: Enhanced monitoring in all CKD stages due to GI effects
Hepatic Impairment
Limited data exists for hepatic dysfunction:
- Mild-moderate impairment: No dose adjustment recommended based on available data
- Severe impairment: Insufficient evidence; use with extreme caution
- Monitoring: Liver function tests at baseline and if symptoms develop
Elderly Populations
Age-related considerations include:
- Similar efficacy: Comparable metabolic benefits across age groups
- Side effect profile: Generally similar, though dehydration risk higher
- Comorbidities: Greater complexity requiring individualized assessment
- Polypharmacy: Increased interaction potential
- Renal function: Age-related decline necessitates monitoring
Pregnancy and Lactation
Critical safety considerations:
- Pregnancy: Contraindicated; discontinue 2 months before planned conception
- Animal studies: Fetal harm observed at high exposures
- Lactation: Unknown excretion in breast milk; not recommended
- Contraception: Reliable methods essential during treatment
Research involving subjects of reproductive potential requires comprehensive contraception counseling and pregnancy testing protocols.
Comparing Tirzepatide Side Effects to Other Peptides
Versus Semaglutide (GLP-1 Agonist)
Direct comparison reveals nuanced differences:
| Side Effect | Tirzepatide | Semaglutide |
|---|---|---|
| Nausea | 18-25% | 20-44% |
| Vomiting | 5-9% | 9-24% |
| Diarrhea | 13-16% | 8-12% |
| Constipation | 6-8% | 3-7% |
| Discontinuation rate | 4-7% | 6-11% |
Some evidence suggests tirzepatide’s dual mechanism may provide better overall tolerability, though individual responses vary considerably[5]. Researchers comparing different peptide formulations should implement standardized adverse event collection methodologies.
Versus Liraglutide (Daily GLP-1 Agonist)
Frequency differences partly reflect dosing schedules:
- Liraglutide: Daily injection, more consistent drug levels
- Tirzepatide: Weekly injection, peak-trough variation
- Nausea: Generally higher with liraglutide (approximately 40%)
- Injection burden: Reduced with weekly tirzepatide
Versus Dual and Triple Agonists in Development
Emerging compounds like retatrutide (GLP-1/GIP/glucagon triple agonist) show:
- Enhanced efficacy: Greater weight loss and metabolic improvements
- Side effect profile: Generally similar GI effects, potentially higher rates
- Tolerability strategies: Similar management approaches applicable
Long-Term Safety Considerations
Cardiovascular Safety
Cardiovascular outcome trials demonstrate:
- SURPASS-CVOT: Ongoing major cardiovascular outcome trial
- Preliminary signals: Potentially favorable cardiovascular effects
- Heart rate: Modest increase (2-4 bpm average)
- Blood pressure: Generally decreased with weight loss
Bone Health
Weight loss medications raise theoretical bone density concerns:
- Mechanism: Rapid weight reduction may affect bone remodeling
- Current evidence: No significant bone density reduction in trials up to 72 weeks
- Monitoring: Consider DEXA scanning in high-risk populations
- Calcium/Vitamin D: Ensure adequate intake during treatment
Nutritional Considerations
Appetite suppression may impact nutrient intake:
- Protein: Ensure adequate intake (0.8-1.2 g/kg) to preserve lean mass
- Micronutrients: Multivitamin supplementation recommended
- Monitoring: Periodic nutritional assessment in long-term protocols
- Dietary counseling: Professional guidance optimizes outcomes
Metabolic Adaptations
Extended GLP-1/GIP receptor stimulation produces adaptations:
- Beta-cell function: Generally improved insulin secretion
- Insulin sensitivity: Enhanced peripheral glucose uptake
- Lipid metabolism: Favorable changes in triglycerides and cholesterol
- Long-term effects: Ongoing research beyond 2-3 years
Monitoring Protocols and Safety Surveillance
Baseline Assessment
Comprehensive evaluation before initiating tirzepatide:
Laboratory tests:
- Complete metabolic panel (renal and hepatic function)
- Lipid panel
- HbA1c and fasting glucose
- Thyroid function (TSH at minimum)
- Amylase/lipase (if pancreatitis risk factors)
- Pregnancy test (reproductive-age females)
Clinical evaluation:
- Medical history (particularly GI, pancreatic, thyroid)
- Medication review (interaction assessment)
- Physical examination
- Baseline vital signs and weight
Ongoing Monitoring
Systematic surveillance during treatment:
Weeks 1-4:
- Weekly symptom assessment
- Hydration status evaluation
- Weight and vital signs
- Glucose monitoring (if diabetic)
Months 2-6:
- Monthly clinical assessment
- Quarterly laboratory monitoring
- Adverse event documentation
- Efficacy parameter tracking
Beyond 6 months:
- Quarterly clinical visits
- Semi-annual comprehensive labs
- Annual thyroid function assessment
- Continuous adverse event surveillance
Adverse Event Documentation
Research protocols should implement standardized reporting:
- Severity grading: Common Terminology Criteria for Adverse Events (CTCAE)
- Causality assessment: Naranjo algorithm or similar validated tool
- Temporal relationship: Precise documentation of onset relative to dosing
- Management interventions: Record all therapeutic approaches
- Outcomes: Resolution, persistence, or progression
Facilities conducting peptide research should establish systematic quality assurance protocols ensuring comprehensive safety monitoring.
Patient Education and Informed Consent
Essential Information Components
Comprehensive education improves outcomes and compliance:
Mechanism explanation:
- How tirzepatide works (dual incretin agonist)
- Expected metabolic effects
- Timeline for therapeutic benefits
Common side effects:
- Detailed GI effect discussion
- Temporal patterns and expected resolution
- Management strategies available
Serious risks:
- Pancreatitis warning signs
- Thyroid concerns and contraindications
- Hypoglycaemia risk (if applicable)
- When to seek immediate medical attention
Practical guidance:
- Injection technique training
- Dietary recommendations
- Hydration importance
- Medication interactions
Informed Consent Considerations
Research protocols require explicit consent addressing:
- Known risks: Comprehensive adverse event profile
- Unknown risks: Limitations of long-term safety data
- Alternative options: Other therapeutic approaches available
- Right to withdraw: Without penalty or prejudice
- Monitoring requirements: Subject responsibilities and commitments
Regulatory Perspectives and Reporting Requirements
FDA and EMA Positions
Regulatory agencies maintain ongoing surveillance:
- Approved indications: Type 2 diabetes (with specific labeling)
- Boxed warnings: Thyroid C-cell tumor risk based on rodent data
- Risk Evaluation and Mitigation Strategy (REMS): Not currently required
- Postmarketing surveillance: Ongoing safety monitoring mandated
Pharmacovigilance Obligations
Healthcare providers and researchers must report:
- Serious adverse events: Death, hospitalization, disability, congenital anomaly
- Unexpected events: Not listed in current labeling
- Medication errors: Particularly those resulting in harm
- Reporting timeframes: Expedited for serious/unexpected events
Research institutions should establish clear pharmacovigilance procedures and designated safety officers.
Emerging Research and Future Directions
Novel Formulations
Development efforts focus on improving tolerability:
- Oral formulations: Potentially different side effect profiles
- Extended-release preparations: Smoother pharmacokinetic profiles
- Combination products: Fixed-dose combinations with complementary agents
Predictive Biomarkers
Research investigating side effect prediction:
- Genetic markers: Polymorphisms affecting drug metabolism or receptor sensitivity
- Baseline characteristics: Clinical and laboratory predictors of tolerance
- Pharmacokinetic monitoring: Correlation between drug levels and adverse events
Mitigation Strategies
Innovative approaches under investigation:
- Prophylactic anti-emetics: Routine use during initiation and escalation
- Alternative dosing schedules: Twice-weekly or every-10-day regimens
- Gradual micro-dosing: Very slow escalation protocols
- Combination therapies: Agents that may offset specific side effects
Researchers exploring advanced peptide applications contribute valuable insights into optimizing therapeutic peptide tolerability across multiple compounds.
Clinical Decision-Making Framework
When to Initiate Tirzepatide
Appropriate candidate characteristics:
Favorable factors:
- Type 2 diabetes inadequately controlled on other agents
- BMI ≥27 with weight-related comorbidities
- No contraindicated conditions
- Realistic expectations regarding side effects
- Commitment to monitoring and follow-up
Concerning factors:
- History of pancreatitis or MEN 2
- Severe gastroparesis
- Active gallbladder disease
- Pregnancy or planned conception
- Inability to comply with monitoring
When to Continue Despite Side Effects
Persistence often warranted when:
- Side effects mild-moderate and improving
- Significant therapeutic benefit evident
- Subject motivated to continue
- Effective management strategies available
- No serious safety signals present
When to Discontinue
Clear discontinuation indications:
- Absolute: Pancreatitis, severe allergic reaction, medullary thyroid cancer diagnosis
- Relative: Intolerable persistent side effects, inadequate efficacy, patient preference
- Temporary: Severe intercurrent illness, planned surgery, pregnancy
Conclusion
Understanding Mounjaro (Tirzepatide) Side Effects: What to Expect empowers researchers, clinicians, and informed stakeholders to make evidence-based decisions regarding this powerful dual incretin agonist. While gastrointestinal effects—particularly nausea, vomiting, and diarrhea—represent the most common adverse events, affecting 30-45% of subjects depending on dose, these typically prove manageable and often diminish substantially within weeks to months of continued exposure.
The dose-dependent nature of tirzepatide’s side effect profile underscores the importance of gradual escalation protocols, allowing physiological adaptation and minimizing adverse event severity. Serious complications, including pancreatitis, thyroid concerns, and hypoglycaemia (when combined with insulin or sulfonylureas), remain relatively rare but necessitate appropriate screening, monitoring, and subject education.
Proactive management strategies—encompassing dietary modifications, hydration protocols, symptomatic pharmacological interventions, and individualized dose adjustments—significantly enhance tolerability and support protocol adherence. The temporal pattern of side effects, with peak incidence during initial exposure and dose escalation periods followed by gradual improvement, provides reassurance that persistence often yields favorable long-term tolerability profiles.
For research institutions and laboratories investigating tirzepatide and related peptide compounds, sourcing high-purity research-grade materials from reputable suppliers ensures experimental validity and safety. Comprehensive safety monitoring, standardized adverse event documentation, and rigorous informed consent processes remain essential components of responsible peptide research protocols.
As the scientific understanding of tirzepatide continues to evolve through ongoing clinical trials and real-world evidence accumulation, the side effect profile will be further refined, predictive factors identified, and mitigation strategies optimized. The current evidence base supports tirzepatide as a generally well-tolerated compound when administered with appropriate clinical oversight, patient selection, and proactive management of anticipated adverse events.
Next Steps:
- For researchers: Establish comprehensive safety monitoring protocols before initiating tirzepatide studies
- For clinicians: Implement systematic patient education and follow-up schedules
- For institutions: Ensure access to high-quality peptide sources and safety resources
- For all stakeholders: Stay informed regarding emerging safety data and evolving best practices
The balance between tirzepatide’s remarkable therapeutic potential and its manageable side effect profile positions this dual incretin agonist as a valuable tool in metabolic research and clinical practice, provided that comprehensive understanding and proactive management of Mounjaro (Tirzepatide) Side Effects: What to Expect guide its responsible application.
References
[1] Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385(6):503-515.
[2] Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes – state-of-the-art. Mol Metab. 2021;46:101102.
[3] Rosenstock J, Wysham C, Frías JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143-155.
[4] Azoulay L, Filion KB, Platt RW, et al. Association Between Incretin-Based Drugs and the Risk of Acute Pancreatitis. JAMA Intern Med. 2016;176(10):1464-1473.
[5] Ludvik B, Giorgino F, Jódar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial. Lancet. 2021;398(10300):583-598.