
1.The Imperative of Precision in Survodutide Dosage Research
In the rapidly evolving landscape of metabolic therapeutics, Survodutide (BI 456906) represents a significant leap forward. Unlike mono-agonists targeting only the GLP-1 receptor, Survodutide functions as a dual agonist, activating both the glucagon receptor (GCGR) and the glucagon-like peptide-1 receptor (GLP-1R). This dual mechanism offers a synergistic approach: the GLP-1 component drives satiety and insulin secretion, while the glucagon component increases energy expenditure through lipid metabolism.
However, this increased potency and complexity introduce significant challenges in a research setting. The inclusion of glucagon receptor agonism narrows the therapeutic window compared to pure GLP-1 agonists. In clinical trials and animal models, the “glucagon effect” can lead to distinct physiological responses, such as elevated heart rate or acute gastrointestinal distress, if introduced too aggressively.
For laboratory researchers, precise dosing is not merely a matter of data accuracy; it is the primary safeguard against “Subject Dropout.” In the context of a study, dropout refers to the necessity of removing a subject (animal model or clinical participant) due to intolerance of the compound. High dropout rates compromise the statistical power of a study and can invalidate months of data collection.
Therefore, the operational handling of Survodutide—from the moment the lyophilized powder is reconstituted to the minute calculation of the escalation schedule—requires a higher degree of rigor than standard peptide protocols. This guide serves as an operational manual for maintaining that rigor, ensuring that the variable in your experiment is the compound’s efficacy, not an error in its administration.
2. Reconstitution Protocols: A Step-by-Step Lab Guide
The stability and efficacy of Survodutide depend heavily on proper reconstitution. Peptides are fragile biological chains; improper handling can lead to denaturation, aggregation, or precipitation, rendering the dose ineffective or causing inflammatory reactions in test subjects.
2.1 Essential Laboratory Supplies
Before retrieving the peptide from storage, ensure the designated biological safety cabinet or clean workspace is prepped with the following:
-
Lyophilized Survodutide: Typically supplied in vacuum-sealed pen peptides containing 2mg, 5mg, or 10mg of powder.
-
Bacteriostatic Water (BAC): Sterile water containing 0.9% benzyl alcohol. The alcohol acts as a preservative, allowing the pen peptide to be used for multiple doses over a period of 28 days (if refrigerated).
-
Note: Use Sterile Water for Injection (SWFI) only if the entire pen peptide will be administered immediately in a single acute study, as it lacks preservatives to prevent bacterial growth over time.
-
-
Insulin Syringes (for administration): Typically U-100, 29G to 31G needles.
-
Reconstitution Syringe: A larger gauge (e.g., 3ml syringe with a 23G or 25G needle) is often preferred for drawing up the diluent to avoid high-pressure streaming which can damage the peptide cake.
-
Alcohol Prep Pads: 70% Isopropyl alcohol for sterilizing pen peptide stoppers.
-
Sharps Container: For immediate disposal of needles.
-
Sterile Gloves: To maintain aseptic technique.
2.2 The “Vacuum Technique” for Pressure Equalization
Most research peptides are lyophilized under a vacuum to ensure stability. When a needle pierces the septum, the vacuum can aggressively “suck” the diluent in. If the stream of water hits the delicate peptide powder directly with high force, it can physically shear the peptide bonds.
The Protocol:
-
Sanitize: Wipe the rubber stoppers of both the Bacteriostatic water pen peptide and the Survodutide pen peptide with separate alcohol pads. Allow them to air dry (approx. 10 seconds).
-
Draw Diluent: Using the reconstitution syringe, draw up the desired volume of Bacteriostatic water (e.g., 1.0 mL or 2.0 mL—see Section 3 for calculations).
-
Release Pressure (The Vacuum Trick):
-
Insert the needle into the Survodutide pen peptide at a 45-degree angle.
-
Do not depress the plunger immediately.
-
Let the pen peptide’s natural vacuum pull the plunger down slowly.
-
Crucial: Aim the needle tip toward the glass wall of the pen peptide, not the powder. The liquid should trickle down the side of the glass and gently rise to submerge the powder.
-
-
Equalize: Once the water is in, if there is still vacuum pressure pulling on the plunger, pull back gently or detach the syringe to allow air to equalize (depending on whether you want positive or neutral pressure storage). Generally, neutral pressure is best for storage to prevent leakage.
2.3 Solubilization Best Practices
Once the diluent is added, the peptide must dissolve completely.
-
Do Not Shake: Never vigorously shake the pen peptide. This creates bubbles (frothing), which denatures proteins and alters the concentration by trapping peptide in the foam.
-
Swirl Gently: Use a gentle “figure-8” motion or roll the pen peptide between your palms.
-
Visual Inspection: The solution should be crystal clear. If it is cloudy or contains particulates after 5 minutes of gentle swirling, the peptide may have degraded or precipitated (“crashed”) and should not be used for research.
3. Mathematical Models: Dosage Calculations
Accurate research relies on converting the mass of the drug (milligrams) into an injectable volume (milliliters). This relationship is defined by the Concentration.
3.1 Establishing a Concentration Standard
In a lab setting, it is best to standardize concentration across all pen peptides to prevent dosing errors during the study.
-
Option A: The High Concentration Approach (for high-dose cohorts)
-
Vial: 5 mg Survodutide
-
Diluent: 1.0 mL Bacteriostatic Water
-
Concentration: $5 mg / 1 mL = 5 mg/mL$
-
Utility: Best for later stages of titration where volumes would otherwise become too large for subcutaneous administration.
-
-
Option B: The Precision Approach (for starting cohorts)
-
Vial: 5 mg Survodutide
-
Diluent: 2.0 mL Bacteriostatic Water
-
Concentration: $5 mg / 2 mL = 2.5 mg/mL$
-
Utility: Allows for finer adjustments at the micro-dose level (e.g., 0.6 mg).
-
3.2 The Calculation Formula
To determine “units” on an insulin syringe or mL volume for a specific dose:
Example Scenario 1: The Starting Dose
-
Target Dose: 0.6 mg
-
Vial Setup: 5 mg peptide in 2 mL water (Concentration: 2.5 mg/mL).
-
Conversion to Insulin Units: $0.24 \text{ mL} \times 100 \text{ units/mL} = \mathbf{24 \text{ Units}}$.
Example Scenario 2: The Phase 2 High Dose
-
Target Dose: 4.8 mg
-
Vial Setup: 10 mg peptide in 2 mL water (Concentration: 5 mg/mL).
-
Conversion to Insulin Units: $\mathbf{96 \text{ Units}}$ (almost a full U-100 syringe).
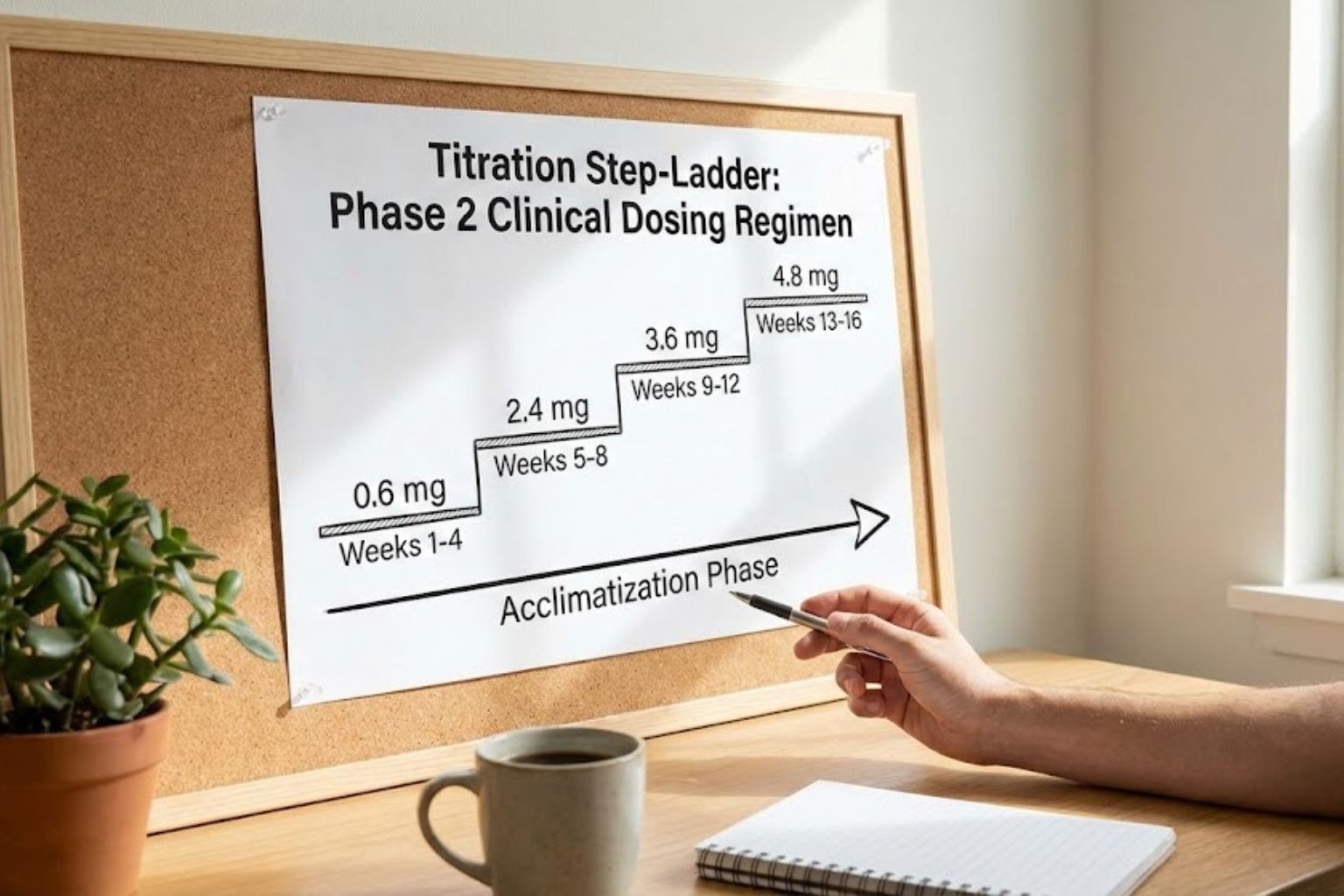
4. Titration Protocols: Escalation Strategies
The most critical operational aspect of researching dual agonists is the titration schedule. Unlike pure GLP-1s, the glucagon component of Survodutide significantly increases metabolic rate and heart rate. Rapid escalation does not lead to faster weight loss in subjects; it leads to severe gastrointestinal rejection and cardiac stress.
4.1 The “Start Low, Go Slow” Philosophy
Clinical trials conducted by Boehringer Ingelheim utilized a cautious escalation strategy. The goal is to allow the subject’s body to upregulate receptor tolerance, specifically mitigating the nausea associated with GLP-1 agonism and the palpitations associated with GCGR agonism.
4.2 Standard Research Escalation Schedule (Based on Clinical Data)
The following schedule assumes a 4-week stabilization period at each dose before escalating. This is the “Gold Standard” for reducing subject dropout.
| Phase | Duration | Dosage (Weekly) | Research Objective |
| Induction | Weeks 1-4 | 0.6 mg | Assess initial tolerance. Monitor for allergic reaction or acute GI distress. |
| Step 1 | Weeks 5-8 | 1.2 mg | First therapeutic threshold. Begin monitoring lipid profiles and glucose levels. |
| Step 2 | Weeks 9-12 | 1.8 mg | Intermediate step. Often skipped in aggressive protocols, but recommended for Survodutide. |
| Step 3 | Weeks 13-16 | 2.4 mg | Common maintenance dose for metabolic health studies. Significant weight reduction usually observed here. |
| Step 4 | Weeks 17-20 | 3.6 mg | High efficacy dose. Close monitoring of resting heart rate is required. |
| Step 5 | Weeks 21+ | 4.8 mg | Maximum Investigated Dose (Phase 2). Used for severe obesity models. |
4.3 Alternative Micro-Dosing Strategies
Some laboratory protocols call for “Micro-Titration” to completely bypass side effects. This involves increasing the dose every 2 weeks by smaller increments rather than doubling the dose every 4 weeks.
-
Week 1-2: 0.6 mg
-
Week 3-4: 0.9 mg
-
Week 5-6: 1.2 mg
-
Week 7-8: 1.5 mg
Advantage: Provides granular data on the minimum effective dose (MED).
Disadvantage: Extends the duration of the study significantly.
5. Handling Adverse Events in Subjects: Operational Adjustments
In a clinical research setting, “Subject Dropout” due to adverse events (AEs) is a failure of protocol. The lab manager must have contingency plans for when subjects react poorly.
5.1 Gastrointestinal Distress (Nausea/Vomiting)
This is the most common AE, driven by the GLP-1 delay in gastric emptying.
-
Protocol Adjustment: If significant nausea occurs upon escalation (e.g., moving from 1.2 mg to 2.4 mg), the protocol dictates de-escalation.
-
Action: Return the subject to the previous tolerated dose (1.2 mg) for an additional 2 weeks before attempting re-escalation.
-
Hydration: Ensure hydration protocols are strictly enforced, as dehydration exacerbates GLP-1 nausea.
5.2 Elevated Heart Rate (Tachycardia)
Driven by the Glucagon receptor’s effect on the sinoatrial node.
-
Monitoring Threshold: In Phase 2 trials, a mean increase of pulse rate (approx. 5–10 bpm) was observed.
-
Safety Cutoff: If a subject exhibits a resting heart rate increase of >20 bpm sustained over 24 hours, the study protocol usually requires cessation of the compound until levels normalize.
5.3 Injection Site Reactions (ISR)
-
Cause: Often due to cold peptide or high alcohol content in the bacteriostatic water.
-
Mitigation: Allow the reconstituted syringe to sit at room temperature for 5–10 minutes before administration (if stable) and ensure the alcohol from the swab has fully evaporated from the skin before needle insertion.
6. Safety Calculations & Verification
Before any injection in a controlled study, a “Safety Check” calculation is mandatory. This prevents the catastrophic “Decimal Error” (e.g., dosing 6.0 mg instead of 0.6 mg).
6.1 The “Rule of Tens” Verification
Always verify the position of the decimal point against the syringe unit markings.
-
If the dose is 0.6 mg and concentration is 2.0 mg/mL:
-
Volume is 0.3 mL.
-
On a U-100 syringe, this is 30 Units.
-
-
Visual Check: Does the liquid volume look appropriate? 30 units is roughly 1/3 of a standard 1mL syringe. If you have filled the whole syringe (100 units/1mL) for a starting dose, you have likely miscalculated by a factor of 3x.
6.2 Labelling Protocols
Once reconstituted, the pen peptide is no longer a generic powder. It is a biological agent with an expiration clock.
-
Label Requirements:
-
Date of Reconstitution.
-
Concentration (e.g., “5mg/2mL”).
-
Initials of the technician.
-
Expiration Date (Standard: 28 days from reconstitution).
-
7. Storage and Stability
7.1 Lyophilized (Powder)
-
Freezer (-20°C): Can be stored for 12–24 months.
-
Room Temperature: Stable for roughly 30 days (keep away from heat/moisture).
-
Light: Keep protected from light.
7.2 Reconstituted (Liquid)
-
Refrigeration (2°C to 8°C): Mandatory.
-
Shelf Life: 28 days maximum. After this, peptide degradation accelerates, and the risk of bacterial contamination (despite benzyl alcohol) increases.
-
Freezing: NEVER freeze reconstituted peptide. The formation of ice crystals destroys the tertiary structure of the peptide, rendering it useless.
8. Precision as the Key to Success
The investigation of Survodutide offers promising avenues for treating obesity and MASH (metabolic dysfunction-associated steatohepatitis). However, the dual-agonist nature of the compound demands a higher standard of laboratory discipline than previous generations of incretin mimetics.
By adhering to the Vacuum Technique for reconstitution, verifying concentration through rigorous Mathematical Models, and strictly following a Slow-Escalation Titration Schedule, researchers can ensure high-fidelity data. In the realm of peptide research, patience and precision are not just safety measures—they are the very instruments of discovery.
Quick Reference: Survodutide Titration Table
| Week | Dose (mg) | Volume (at 2.5mg/mL conc.) | Insulin Units (U-100) |
| 1-4 | 0.6 mg | 0.24 mL | 24 Units |
| 5-8 | 1.2 mg | 0.48 mL | 48 Units |
| 9-12 | 1.8 mg | 0.72 mL | 72 Units |
| 13-16 | 2.4 mg | 0.96 mL | 96 Units |
| 17+ | Switch to 5mg/mL Conc. | Recalculate | Recalculate |
Troubleshooting Guide
| Issue | Probable Cause | Solution |
| Cloudy Solution | Peptide crashed/Water pH issue | Discard pen peptide. Do not inject. |
| Vacuum Hiss Missing | Seal compromised | Vial may be non-sterile. Discard. |
| Severe Nausea | Dose escalated too fast | Skip next dose, return to lower dose. |
| Hard Lump at Site | Subcutaneous leak/Reaction | Rotate injection sites strictly. |
Disclaimer: The following information is strictly for educational and informational purposes regarding laboratory research and development. Survodutide is a compound currently under clinical investigation and is not approved for general medical use. This guide describes protocols for handling, reconstitution, and dosage titration in a professional laboratory setting (in vitro or in vivo animal studies). It does not constitute medical advice, nor does it encourage the use of research chemicals on humans outside of authorized clinical trials.