When working with research-grade peptides, precision matters. Understanding tirzepatide dose in units is essential for researchers conducting controlled studies with this dual GIP/GLP-1 receptor agonist. Whether you’re calibrating protocols, converting milligram doses to insulin syringe measurements, or establishing consistent administration schedules, accurate unit calculations prevent costly errors and ensure reproducible results. This comprehensive guide demystifies tirzepatide dosing conversions, providing the mathematical frameworks and practical techniques that laboratory professionals need for precise peptide research.
Key Takeaways
- Tirzepatide dose in units depends entirely on reconstitution volume—the same milligram dose yields different unit measurements based on bacteriostatic water added
- Standard insulin syringes (100-unit capacity) provide the most accurate measurement tool for research peptide administration when properly calibrated
- Common research doses range from 2.5mg to 15mg, with unit measurements varying from 5 to 60 units depending on concentration protocols
- Proper calculation formula: (Desired dose in mg ÷ Total peptide in pen peptide) × Total reconstitution volume in units = Units to draw
- Maintaining detailed dosing logs with reconstitution volumes, concentrations, and unit conversions ensures research consistency and reproducibility
Understanding Tirzepatide Dosing Fundamentals
Tirzepatide represents a significant advancement in peptide research, functioning as a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist. For researchers working with this compound, understanding how to accurately measure and administer doses is paramount to experimental integrity.
What Are “Units” in Peptide Dosing?
In peptide research, “units” typically refer to the measurement markings on insulin syringes, which are calibrated in 100 equal divisions. Each marking represents one unit, with the entire syringe holding 1ml (100 units) of liquid. The critical concept: units are volume measurements, not weight measurements. The relationship between milligrams (weight) and units (volume) depends entirely on concentration—how much peptide powder you dissolve in how much liquid.
When researchers discuss tirzepatide dose in units, they’re describing the volume of reconstituted solution needed to deliver a specific milligram dose. This conversion is not standardized; it varies based on individual reconstitution protocols.
Why Unit Conversion Matters for Research
Precision in peptide research cannot be overstated. Unlike pharmaceutical preparations with pre-measured doses, research-grade peptides from suppliers like PEPTIDE PRO arrive as lyophilized powder requiring reconstitution. Researchers must:
- Calculate accurate concentrations based on peptide amount and bacteriostatic water volume
- Convert desired milligram doses into measurable syringe units
- Maintain consistency across experimental timeframes
- Document protocols for reproducibility
Errors in unit conversion can result in under-dosing (compromising research outcomes) or over-dosing (wasting valuable compounds and potentially skewing results). For high-value peptides, precision directly impacts both scientific validity and research budgets.
The Relationship Between Milligrams and Units
The fundamental equation governing tirzepatide dose in units is straightforward:
Concentration = Total Peptide (mg) ÷ Reconstitution Volume (ml)
Once concentration is established, converting any desired dose to units follows this formula:
(Desired Dose in mg ÷ Concentration in mg/ml) × 100 = Units to Draw
Alternatively:
(Desired Dose in mg ÷ Total Peptide in Vial) × Total Reconstitution Volume in Units = Units to Draw
This mathematical relationship means that the same 5mg dose of tirzepatide could be 10 units, 20 units, or 50 units depending on how the pen peptide was reconstituted—there is no universal “units per milligram” standard.
Calculating Tirzepatide Dose in Units: Step-by-Step Methods
Accurate calculation of tirzepatide dose in units requires systematic methodology. This section provides detailed protocols for converting milligram doses to syringe measurements across various reconstitution scenarios.
Standard Reconstitution Volumes and Concentrations
Most researchers use bacteriostatic water in volumes between 1ml and 3ml for peptide reconstitution, balancing concentration (higher with less water) against ease of measurement (easier with more water).
Common Tirzepatide Reconstitution Examples:
| Vial Size | Bacteriostatic Water | Concentration | 2.5mg Dose | 5mg Dose | 10mg Dose |
|---|---|---|---|---|---|
| 10mg | 1ml (100 units) | 10mg/ml | 25 units | 50 units | 100 units |
| 10mg | 2ml (200 units) | 5mg/ml | 50 units | 100 units | N/A |
| 20mg | 2ml (200 units) | 10mg/ml | 25 units | 50 units | 100 units |
| 30mg | 2ml (200 units) | 15mg/ml | 16.7 units | 33.3 units | 66.7 units |
| 30mg | 3ml (300 units) | 10mg/ml | 25 units | 50 units | 100 units |
| 40mg | 2ml (200 units) | 20mg/ml | 12.5 units | 25 units | 50 units |
| 50mg | 2ml (200 units) | 25mg/ml | 10 units | 20 units | 40 units |
Notice how the same 5mg dose ranges from 20 units (50mg pen peptide with 2ml water) to 100 units (10mg pen peptide with 2ml water). This variability underscores why researchers must calculate conversions for their specific reconstitution protocol.
The Universal Calculation Formula
For any tirzepatide pen peptide and reconstitution volume, use this reliable formula:
Units to Draw = (Desired Dose ÷ Total Peptide) × Reconstitution Volume in Units
Example 1: You have a 30mg tirzepatide pen peptide reconstituted with 2ml bacteriostatic water, and you need a 7.5mg dose.
- Desired Dose: 7.5mg
- Total Peptide: 30mg
- Reconstitution Volume: 2ml = 200 units
Calculation: (7.5 ÷ 30) × 200 = 0.25 × 200 = 50 units
Example 2: You have a 10mg pen peptide reconstituted with 1ml water, and you need a 2.5mg dose.
- Desired Dose: 2.5mg
- Total Peptide: 10mg
- Reconstitution Volume: 1ml = 100 units
Calculation: (2.5 ÷ 10) × 100 = 0.25 × 100 = 25 units
Creating Your Personal Dosing Chart
For ongoing research protocols, creating a reference chart eliminates repeated calculations and reduces error risk. Document:
- Vial Information: Total peptide amount, batch number, reconstitution date
- Reconstitution Details: Volume of bacteriostatic water added, final concentration
- Dose Conversion Table: All planned doses with corresponding unit measurements
- Visual Syringe Guide: Marked diagrams showing where each dose falls on syringe scale
Many researchers laminate these charts and keep them with their peptide storage area for quick reference. When working with multiple peptides from PEPTIDE PRO’s extensive catalogue, maintaining separate charts for each compound prevents cross-contamination of protocols.
Digital Calculators and Verification Tools
While manual calculation builds understanding, digital tools provide verification and speed for routine work. Several peptide dosing calculators are available online, requiring inputs for:
- Total peptide in pen peptide (mg)
- Reconstitution volume (ml)
- Desired dose (mg)
The calculator returns units to draw. Important: Always verify calculator results with manual calculation for your first few uses to ensure you understand the underlying mathematics. Technology assists but should not replace fundamental comprehension.
Common Calculation Mistakes to Avoid
❌ Mistake #1: Confusing total pen peptide content with concentration A 30mg pen peptide is not “30mg/ml” unless reconstituted with exactly 1ml water.
❌ Mistake #2: Forgetting to convert milliliters to units 2ml = 200 units, not 2 units. Always multiply ml by 100 for insulin syringe measurements.
❌ Mistake #3: Using outdated reconstitution information If you add more bacteriostatic water to a partially used pen peptide, all previous unit calculations become invalid.
❌ Mistake #4: Rounding too aggressively Maintain at least one decimal place in intermediate calculations; round only the final unit measurement.
✅ Best Practice: Calculate twice, draw once. Verify your math before drawing from the pen peptide, especially when working with high-value research compounds.
Practical Administration: From Calculation to Injection
Understanding tirzepatide dose in units mathematically is only half the equation—accurate physical measurement and administration complete the protocol. This section covers practical techniques for precise peptide handling in research settings.
Selecting the Right Syringe for Unit Measurement
Insulin syringes are the gold standard for peptide research administration due to their:
- Precise calibration: 100-unit capacity with clear markings
- Fine gauge needles: Typically 29-31 gauge for minimal tissue trauma
- Fixed needle design: Eliminates dead space found in detachable needle systems
- Volume capacity: 0.3ml, 0.5ml, or 1ml options for different dose ranges
Syringe Selection Guidelines:
| Dose Range | Recommended Syringe | Rationale |
|---|---|---|
| 5-30 units | 0.3ml (30-unit) | Maximum precision for small volumes |
| 30-50 units | 0.5ml (50-unit) | Good balance of precision and capacity |
| 50-100 units | 1ml (100-unit) | Full range, standard choice for most protocols |
⚠️ Critical Note: Never use tuberculin syringes or other non-insulin syringes for unit-based dosing. Their markings represent different volumes and will result in significant dosing errors.
Drawing the Correct Dose: Step-by-Step Technique
Proper aseptic technique protects both the researcher and the peptide integrity. Follow this protocol when working with reconstituted tirzepatide or other research peptides:
Preparation Phase:
- Wash hands thoroughly and consider wearing nitrile gloves
- Gather supplies: alcohol swabs, insulin syringe, peptide pen peptide, sharps container
- Remove pen peptide from refrigerated storage (2-8°C)
- Allow pen peptide to reach room temperature (10-15 minutes) to reduce bubble formation
- Verify pen peptide label, concentration, and unit calculation
Drawing Phase:
- Wipe pen peptide rubber stopper with alcohol swab and allow to dry (15 seconds)
- Remove syringe from sterile packaging without touching needle
- Pull plunger to draw air equal to your dose in units
- Insert needle through rubber stopper at 90-degree angle
- Inject air into pen peptide to prevent vacuum formation
- Invert pen peptide (needle tip submerged in liquid)
- Slowly pull plunger to slightly beyond target unit marking
- Check for air bubbles; if present, tap syringe gently and push bubbles back into pen peptide
- Adjust plunger to exact unit marking at eye level
- Withdraw needle from pen peptide and recap carefully using one-handed scoop technique
Verification:
- Double-check unit measurement against calculation
- Inspect solution for clarity (should be clear, no particulates)
- Confirm no air bubbles remain in syringe
- Document dose drawn in research log
Subcutaneous Administration Protocols
For research involving subcutaneous administration, proper technique ensures consistent absorption and minimal subject discomfort:
Site Selection:
- Abdomen (2 inches from navel, avoiding midline)
- Anterior thigh
- Upper arm (outer aspect)
- Rotate sites systematically to prevent lipohypertrophy
Administration Steps:
- Clean injection site with alcohol swab in outward spiral motion
- Allow skin to dry completely (prevents stinging)
- Pinch skin fold between thumb and forefinger
- Insert needle at 45-90 degree angle (depending on subject adipose tissue)
- Release skin pinch
- Inject slowly and steadily (5-10 seconds for full dose)
- Wait 5 seconds before withdrawing needle
- Withdraw at same angle as insertion
- Apply gentle pressure with clean gauze (do not rub)
- Dispose of syringe immediately in sharps container
Handling Partial Units and Dose Adjustments
Research protocols often require doses that fall between syringe markings. For example, a calculated dose of 33.3 units for a 5mg dose from a 30mg pen peptide reconstituted with 2ml water.
Strategies for precision:
Rounding Method: Round to nearest whole or half unit marking
- 33.3 units → 33 units (0.5% underdose)
- Acceptable for most research applications where minor variance is tolerable
Reconstitution Adjustment: Modify bacteriostatic water volume to yield whole-unit doses
- Instead of 2ml, use 1.8ml (180 units) for the 30mg pen peptide
- 5mg dose = (5 ÷ 30) × 180 = 30 units exactly
Syringe Technique: For half-unit precision
- Use 0.5ml syringes with 50 half-unit markings
- Provides double the precision of standard 1ml syringes
Documentation Protocol: Record actual administered dose
- If calculation yields 33.3 units but you draw 33 units, document: “Calculated: 33.3u, Administered: 33u (4.995mg actual)”
Storage and Stability Considerations
Proper storage maintains peptide integrity and ensures dose accuracy throughout research protocols:
Lyophilized (Unreconstituted) Peptides:
- Store at -20°C or colder
- Protect from light and moisture
- Stable for extended periods (typically 2+ years)
- Allow to reach room temperature before opening to prevent condensation
Reconstituted Peptides:
- Store at 2-8°C (standard refrigerator)
- Protect from light (amber pen peptides or foil wrap)
- Use within 28-60 days depending on peptide (check PEPTIDE PRO documentation)
- Never freeze reconstituted solutions
- Label with reconstitution date and concentration
Pre-Drawn Syringes:
- Generally not recommended for research peptides
- If necessary, refrigerate and use within 24 hours
- Increased contamination and degradation risk
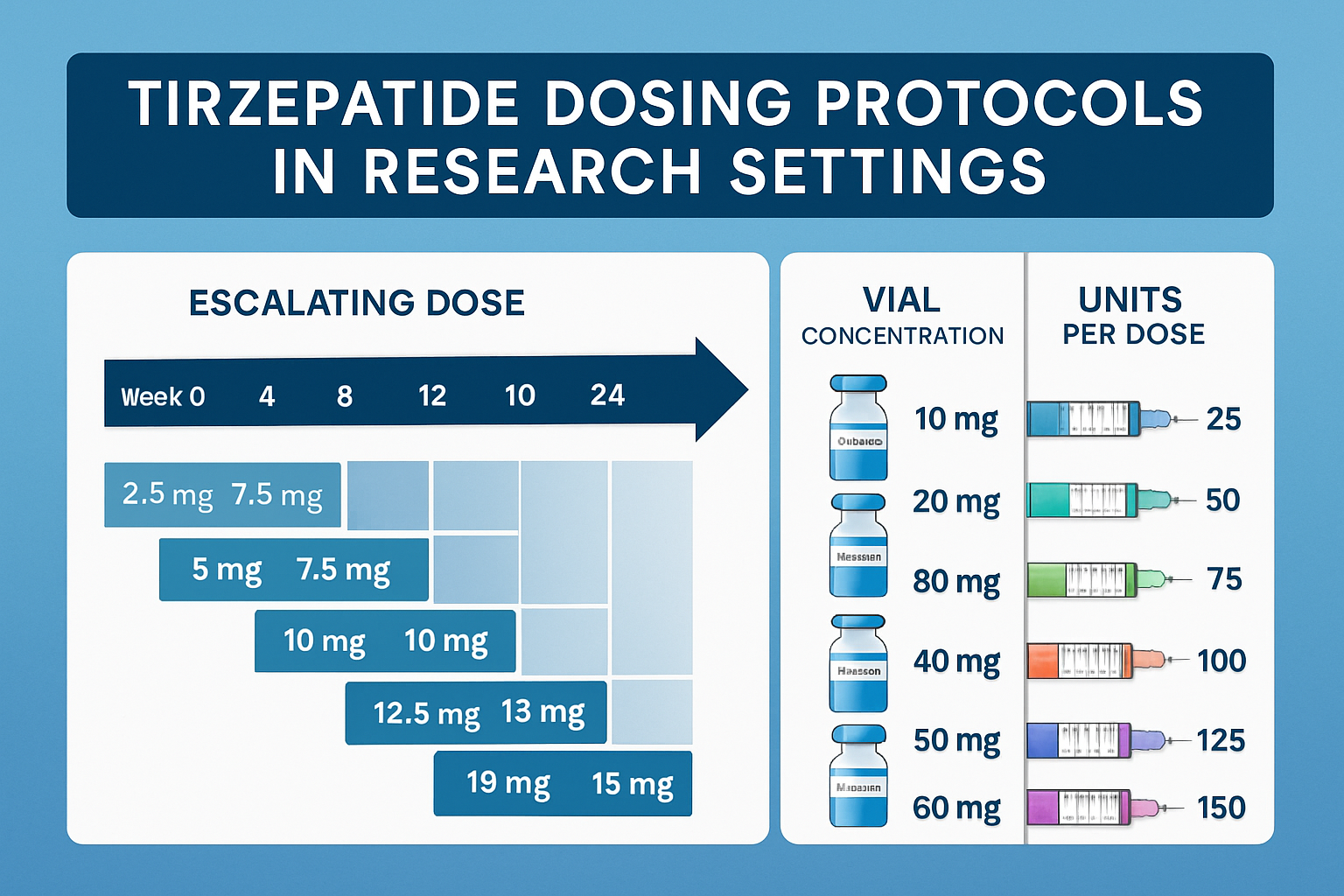
Dose Escalation Protocols and Unit Conversions
Research with tirzepatide frequently involves graduated dosing schedules, requiring systematic tirzepatide dose in units conversions across multiple administration levels. Understanding escalation protocols ensures smooth transitions between doses while maintaining measurement accuracy.
Standard Research Dose Progression
Tirzepatide research typically follows escalating dose protocols to assess tolerance and optimize outcomes. Common progression schedules include:
Conservative Escalation (4-week intervals):
- Weeks 1-4: 2.5mg
- Weeks 5-8: 5mg
- Weeks 9-12: 7.5mg
- Weeks 13-16: 10mg
- Weeks 17-20: 12.5mg
- Weeks 21+: 15mg
Moderate Escalation (2-week intervals):
- Weeks 1-2: 2.5mg
- Weeks 3-4: 5mg
- Weeks 5-6: 7.5mg
- Weeks 7-8: 10mg
- Weeks 9-10: 12.5mg
- Weeks 11+: 15mg
Each dose level requires recalculation of tirzepatide dose in units based on your specific pen peptide concentration. Creating a comprehensive conversion table before beginning research prevents mid-protocol calculation errors.
Multi-Vial Protocol Planning
Longer research protocols often require multiple pen peptides as doses escalate. Strategic planning optimizes peptide usage and minimizes waste:
Example Protocol: 24-Week Study with Conservative Escalation
Phase 1 (Weeks 1-8): 2.5mg and 5mg doses
- Option A: Use 10mg pen peptide with 2ml water (5mg/ml concentration)
- 2.5mg = 50 units (4 doses per pen peptide)
- 5mg = 100 units (2 doses per pen peptide)
- Total needed: 2 pen peptides for 8 weeks
Phase 2 (Weeks 9-16): 7.5mg and 10mg doses
- Option B: Use 30mg pen peptide with 2ml water (15mg/ml concentration)
- 7.5mg = 50 units (4 doses per pen peptide)
- 10mg = 66.7 units (3 doses per pen peptide)
- Total needed: 2 pen peptides for 8 weeks
Phase 3 (Weeks 17-24): 12.5mg and 15mg doses
- Option C: Use 40mg pen peptide with 2ml water (20mg/ml concentration)
- 12.5mg = 62.5 units (3 doses per pen peptide)
- 15mg = 75 units (2.6 doses per pen peptide)
- Total needed: 3 pen peptides for 8 weeks
Budget Optimization: Larger pen peptides typically offer better cost-per-milligram ratios, but only if the full pen peptide content will be used within stability windows.
Unit Conversion Tables for Common Escalation Schedules
For researchers using standard 2ml reconstitution volumes, these reference tables provide quick tirzepatide dose in units conversions:
30mg Vial + 2ml Water (15mg/ml concentration):
| Dose (mg) | Units to Draw | Doses per Vial |
|---|---|---|
| 2.5 | 16.7 (≈17) | 12 |
| 5.0 | 33.3 (≈33) | 6 |
| 7.5 | 50.0 | 4 |
| 10.0 | 66.7 (≈67) | 3 |
| 12.5 | 83.3 (≈83) | 2.4 |
| 15.0 | 100.0 | 2 |
50mg Vial + 2ml Water (25mg/ml concentration):
| Dose (mg) | Units to Draw | Doses per Vial |
|---|---|---|
| 2.5 | 10.0 | 20 |
| 5.0 | 20.0 | 10 |
| 7.5 | 30.0 | 6.7 |
| 10.0 | 40.0 | 5 |
| 12.5 | 50.0 | 4 |
| 15.0 | 60.0 | 3.3 |
60mg Vial + 2ml Water (30mg/ml concentration):
| Dose (mg) | Units to Draw | Doses per Vial |
|---|---|---|
| 2.5 | 8.3 (≈8) | 24 |
| 5.0 | 16.7 (≈17) | 12 |
| 7.5 | 25.0 | 8 |
| 10.0 | 33.3 (≈33) | 6 |
| 12.5 | 41.7 (≈42) | 4.8 |
| 15.0 | 50.0 | 4 |
Maintaining Dosing Consistency During Transitions
When escalating doses, maintaining consistent administration timing and technique ensures valid comparative results:
📋 Escalation Best Practices:
✅ Schedule consistency: Administer at same time of day (±2 hours)
✅ Transition documentation: Record exact date and time of first elevated dose
✅ Observation periods: Monitor for 72 hours post-escalation for tolerance assessment
✅ Calculation verification: Recalculate and verify units before each new dose level
✅ Vial tracking: Label pen peptides clearly with concentration to prevent confusion when using multiple strengths
✅ Protocol adherence: Resist temptation to accelerate escalation schedule without documented justification
Adjusting for Individual Response Variations
Research protocols may require dose modifications based on individual subject responses. Understanding tirzepatide dose in units conversions enables flexible dosing:
Intermediate Doses (between standard levels):
- 3.75mg (between 2.5mg and 5mg)
- 6.25mg (between 5mg and 7.5mg)
- 8.75mg (between 7.5mg and 10mg)
Example: For 6.25mg from a 30mg pen peptide with 2ml water:
- Calculation: (6.25 ÷ 30) × 200 = 41.7 units
- Draw: 42 units (actual dose: 6.3mg)
Dose Reduction Protocols: If tolerance issues arise, systematic reduction follows reverse escalation:
- From 10mg → 7.5mg (25% reduction)
- From 7.5mg → 5mg (33% reduction)
- From 5mg → 2.5mg (50% reduction)
Maintaining detailed logs of all dose adjustments, including calculated units and actual administered volumes, creates valuable data for protocol refinement and publication.
Advanced Considerations for Research Applications
Beyond basic tirzepatide dose in units calculations, sophisticated research protocols require understanding of concentration optimization, combination therapies, and quality assurance measures that ensure experimental validity.
Optimizing Reconstitution Volume for Specific Protocols
The volume of bacteriostatic water used for reconstitution significantly impacts both measurement precision and peptide stability. Strategic volume selection enhances research outcomes:
High-Concentration Protocols (Less Water):
Advantages:
- Smaller injection volumes (more comfortable for subjects)
- Extended pen peptide lifespan (fewer needle punctures)
- Reduced refrigerator storage space
Disadvantages:
- Less precise unit measurements (smaller unit increments represent larger mg amounts)
- Higher viscosity (slightly more difficult to draw)
- Increased concentration may affect stability for some peptides
Example: 50mg pen peptide + 1ml water = 50mg/ml
- 10mg dose = 20 units (very precise)
- 12.5mg dose = 25 units (exact measurement)
Low-Concentration Protocols (More Water):
Advantages:
- Maximum measurement precision (more units per mg)
- Easier to draw (lower viscosity)
- Better for protocols requiring frequent small dose adjustments
Disadvantages:
- Larger injection volumes
- More frequent pen peptide access (potentially increased contamination risk)
- May exceed single-syringe capacity for higher doses
Example: 30mg pen peptide + 3ml water = 10mg/ml
- 10mg dose = 100 units (fills entire 1ml syringe)
- 12.5mg dose = 125 units (requires 0.5ml syringe or two injections)
Optimal Balance: Most researchers find 2ml reconstitution volume provides the best compromise between precision and practicality for tirzepatide across standard dose ranges.
Combination Peptide Protocols and Unit Management
Advanced research often involves multiple peptides administered concurrently. When working with tirzepatide alongside other compounds from PEPTIDE PRO’s research portfolio, maintaining separate calculation systems prevents cross-contamination of protocols.
Common Tirzepatide Combinations in Research:
Tirzepatide + BPC-157:
- Different reconstitution volumes and concentrations
- Separate administration sites
- Independent unit calculation charts
- Distinct storage locations
Tirzepatide + CJC-1295:
- Potential synergistic effects in growth hormone research
- Non-overlapping administration timing
- Separate syringe types if different volumes required
Protocol Organization Strategies:
- Color-coded labels: Different colors for each peptide pen peptide and calculation chart
- Separate storage containers: Individual bins for each compound’s supplies
- Distinct administration logs: Separate documentation prevents data mixing
- Cross-reference tracking: Note interactions and timing relationships
Quality Assurance and Verification Procedures
Professional research protocols incorporate systematic verification to ensure tirzepatide dose in units accuracy throughout extended studies:
Pre-Administration Checklist:
☑
️ Vial identity confirmed (peptide name, concentration, batch number)
☑
️ Expiration and reconstitution dates verified
☑
️ Calculation reviewed (desired mg dose → units to draw)
☑
️ Syringe type confirmed (insulin syringe, appropriate capacity)
☑
️ Visual inspection (solution clarity, no particulates)
☑
️ Unit measurement verified at eye level
☑
️ Documentation prepared (log sheet, timestamp)
Periodic Calibration Verification: Every 10-20 administrations, verify measurement accuracy:
- Draw calculated dose into syringe
- Expel into pre-weighed sterile container
- Weigh solution (should match expected volume: 1ml = 1g)
- Calculate actual peptide amount based on concentration
- Compare to intended dose (should be within ±2%)
Batch Documentation: Maintain comprehensive records for each peptide pen peptide:
- Supplier and batch number (critical for PEPTIDE PRO quality tracking)
- Receipt date and storage conditions
- Reconstitution date, time, and volume
- Concentration calculation
- All doses drawn with dates and unit measurements
- Remaining volume estimates
- Disposal date and method
Temperature and Handling Impact on Dosing Accuracy
Environmental factors affect both peptide stability and measurement precision:
Temperature Considerations:
Cold Solutions (Directly from Refrigerator):
- Higher viscosity → harder to draw accurately
- Air bubbles form more readily
- May cause discomfort upon administration
- Best Practice: Allow pen peptide to reach room temperature 10-15 minutes before drawing
Room Temperature Solutions:
- Optimal viscosity for accurate measurement
- Minimal bubble formation
- More comfortable administration
- Limitation: Should not remain at room temperature >30 minutes
Warm Solutions (>25°C):
- Accelerated degradation potential
- Altered concentration through evaporation (if pen peptide seal compromised)
- Avoid: Never intentionally warm peptide solutions
Humidity and Condensation: When removing cold pen peptides from refrigeration, condensation can form on exterior surfaces. This doesn’t affect internal solution but can:
- Obscure label information
- Make pen peptide slippery (drop risk)
- Introduce moisture to storage area
Prevention: Store pen peptides in sealed containers within refrigerator; allow sealed container to reach room temperature before opening.
Troubleshooting Common Dosing Challenges
Even experienced researchers encounter measurement challenges. Systematic troubleshooting maintains protocol integrity:
Challenge 1: Inconsistent Unit Measurements Between Doses
Possible Causes:
- Vial held at different angles during drawing
- Incomplete bubble removal
- Parallax error (reading units from wrong angle)
- Plunger sticking or inconsistent movement
Solutions:
- Standardize pen peptide position (always fully inverted)
- Tap syringe consistently before final adjustment
- Read measurement at exact eye level
- Use fresh syringes (never reuse)
Challenge 2: Vial Running Out Before Expected
Possible Causes:
- Calculation error in doses per pen peptide
- Overfilling syringes (drawing beyond target)
- Dead space loss in pen peptide
- Evaporation (compromised seal)
Solutions:
- Recalculate expected doses and verify against log
- Implement verification step (second person checks unit measurement)
- Account for ~0.1-0.2ml dead space in planning
- Inspect pen peptide seals; replace if damaged
Challenge 3: Difficulty Drawing Solution (High Resistance)
Possible Causes:
- Vacuum in pen peptide (insufficient air replacement)
- High concentration (viscosity)
- Needle gauge too fine
- Crystallization or precipitation
Solutions:
- Inject air equal to volume being withdrawn
- Use slightly larger needle gauge (28G instead of 31G)
- Verify solution clarity; discard if cloudy or crystallized
- Ensure complete dissolution after reconstitution
Challenge 4: Uncertainty About Remaining Doses
Possible Causes:
- Incomplete logging
- Irregular dose amounts
- Unclear initial volume
Solutions:
- Maintain meticulous dose log (date, units drawn, remaining doses)
- Mark pen peptide with each administration (tally marks)
- Calculate and label “doses remaining” after each use
- When uncertain, reconstitute fresh pen peptide rather than risk underdosing
Regulatory, Safety, and Documentation Standards
Professional research with tirzepatide demands rigorous adherence to documentation protocols, safety standards, and regulatory compliance—particularly when calculating and administering tirzepatide dose in units in controlled research environments.
Research-Only Designation and Compliance
All peptides supplied by PEPTIDE PRO are clearly labeled “For Research Use Only” and are not intended for human consumption or therapeutic use. This designation carries specific implications for handling and documentation:
Regulatory Framework:
- Research-grade peptides are governed by laboratory chemical regulations
- Not subject to pharmaceutical manufacturing standards (GMP)
- Require institutional oversight (ethics committees, safety boards)
- Must be stored, handled, and disposed of according to laboratory protocols
Documentation Requirements:
- Institutional approval documentation
- Research protocol descriptions
- Informed consent (if applicable to research model)
- Detailed administration logs
- Adverse event reporting systems
- Final disposition records
Researcher Responsibilities:
- Verify institutional authorization before procurement
- Maintain separation between research and clinical activities
- Ensure all personnel understand research-only designation
- Implement appropriate safety and containment measures
Laboratory Safety Protocols for Peptide Handling
Working with research peptides requires standard laboratory safety practices:
Personal Protective Equipment (PPE):
- Nitrile gloves (latex-free to prevent allergic reactions)
- Safety glasses (when handling powders or during reconstitution)
- Lab coat (dedicated to peptide work area)
- Closed-toe shoes
Containment Measures:
- Designated peptide preparation area (clean, organized workspace)
- Spill kit readily available (absorbent materials, disinfectant)
- Sharps containers (rigid, puncture-proof, properly labeled)
- Biohazard waste disposal (if applicable to research model)
Hygiene Practices:
- Hand washing before and after handling
- No eating, drinking, or cosmetic application in peptide areas
- Proper aseptic technique for reconstitution
- Regular workspace decontamination
Emergency Procedures:
- Skin contact: Wash immediately with soap and water for 15 minutes
- Eye contact: Flush with water for 15 minutes; seek medical attention
- Ingestion: Do not induce vomiting; seek immediate medical attention
- Spill: Contain area, absorb with appropriate materials, decontaminate surface
Comprehensive Documentation Systems
Professional research demands meticulous record-keeping that extends beyond simple dose logs:
Master Inventory Log: Track all peptide acquisitions and disposals:
- Peptide name and batch number
- Supplier (e.g., PEPTIDE PRO)
- Quantity and concentration
- Receipt date
- Storage location
- Reconstitution date
- Disposal date and method
- Responsible researcher
Reconstitution Record: Document each pen peptide preparation:
- Vial identifier (batch + sequential number)
- Peptide amount (mg)
- Bacteriostatic water volume (ml)
- Final concentration (mg/ml)
- Date and time of reconstitution
- Researcher initials
- Expected expiration date
- Storage conditions
Administration Log: Record every dose with precision:
- Date and time
- Subject identifier
- Vial used (batch + number)
- Intended dose (mg)
- Calculated units
- Actual units drawn
- Administration site
- Any observations or deviations
- Researcher signature
Calculation Verification Log: Maintain records of tirzepatide dose in units calculations:
- Dose level (mg)
- Vial concentration (mg/ml)
- Calculation formula used
- Result (units to draw)
- Verification method (second calculation, digital tool)
- Date and researcher
Quality Control Log: Track verification activities:
- Calibration checks (dates and results)
- Visual inspections (solution clarity)
- Temperature monitoring (storage conditions)
- Expiration date reviews
- Corrective actions taken
Data Integrity and Audit Readiness
Research documentation must withstand scrutiny from institutional review boards, funding agencies, and peer reviewers:
ALCOA+ Principles for Research Data:
- Attributable: Every entry signed/initialed by responsible researcher
- Legible: Clear handwriting or typed entries (no abbreviations without key)
- Contemporaneous: Recorded at time of activity (not retrospectively)
- Original: Primary records retained (copies clearly marked)
- Accurate: Verified and cross-checked
- Complete: All planned data points captured
- Consistent: Standardized formats and terminology
- Enduring: Stored in archival-quality formats
- Available: Accessible for authorized review
Audit Trail Requirements:
- Original entries never obscured (single line through errors, initialed)
- Amendments dated and explained
- Version control for electronic records
- Backup systems for digital data
- Retention period compliance (typically 3-7 years post-publication)
Disposal and Waste Management Protocols
Proper disposal of peptides, solutions, and sharps maintains safety and regulatory compliance:
Unused/Expired Peptide Solutions:
- Do not pour down drains (environmental contamination risk)
- Collect in designated chemical waste containers
- Label with contents and hazard information
- Arrange disposal through institutional chemical waste program
- Document disposal in inventory log
Sharps Disposal:
- Use rigid, puncture-proof sharps containers
- Never recap needles (increased needlestick risk)
- Fill containers only to marked line (typically 75%)
- Seal and label when full
- Dispose through approved medical waste service
- Maintain disposal records
Contaminated Materials:
- Gloves, alcohol swabs, pen peptide packaging
- Dispose in biohazard bags if applicable
- Otherwise, general laboratory waste
- Follow institutional waste segregation protocols
Documentation Requirements:
- Waste disposal logs
- Manifests from disposal services
- Certificates of destruction (for controlled substances)
- Annual waste generation reports (if required)
Mastering Tirzepatide Dose in Units for Research Excellence
Precise understanding of tirzepatide dose in units forms the foundation of rigorous peptide research. As this comprehensive guide has demonstrated, accurate dosing requires more than simple arithmetic—it demands systematic methodology, quality verification, and meticulous documentation that together ensure experimental validity and reproducibility.
Key Principles Reviewed
Mathematical Foundation: The relationship between milligrams and units is entirely dependent on reconstitution volume. There is no universal conversion; each researcher must calculate based on their specific protocol using the formula: (Desired Dose ÷ Total Peptide) × Reconstitution Volume in Units = Units to Draw.
Practical Precision: Insulin syringes calibrated in 100 units provide the optimal measurement tool for research peptide administration. Proper drawing technique, bubble elimination, and eye-level verification ensure accuracy within acceptable research tolerances.
Protocol Optimization: Strategic selection of pen peptide sizes and reconstitution volumes balances measurement precision against practical considerations like injection volume and pen peptide longevity. Most researchers find 2ml bacteriostatic water provides optimal results across standard tirzepatide dose ranges.
Documentation Excellence: Professional research demands comprehensive record-keeping that captures every aspect of peptide handling—from procurement through disposal. These records support research integrity, enable protocol replication, and satisfy regulatory requirements.
Safety Compliance: Research-grade peptides from PEPTIDE PRO are strictly for laboratory use. Proper handling, storage, and disposal protocols protect researchers, maintain compound integrity, and ensure regulatory compliance.
Actionable Next Steps for Researchers
For Researchers Beginning Tirzepatide Protocols:
- Determine your dose escalation schedule based on research objectives and timeline
- Calculate total peptide requirements across the full protocol duration
- Select appropriate pen peptide sizes from PEPTIDE PRO’s tirzepatide options that minimize waste while maintaining stability windows
- Create comprehensive dose conversion charts for your specific reconstitution volumes before beginning research
- Establish documentation systems including inventory logs, reconstitution records, and administration tracking
- Verify calculations using both manual methods and digital tools before first administration
- Implement quality control procedures including periodic calibration verification
For Researchers Optimizing Existing Protocols:
- Review current conversion accuracy by comparing intended versus actual doses administered
- Assess reconstitution volume efficiency—could different volumes improve precision or reduce waste?
- Audit documentation completeness—are all ALCOA+ principles satisfied?
- Evaluate pen peptide size selection—are you optimizing cost-per-dose while respecting stability limits?
- Standardize procedures across research team members to reduce variability
- Implement peer verification for calculations and unit measurements
Resources for Continued Learning
PEPTIDE PRO Educational Materials:
- Reconstitution and storage guidance for all research peptides
- Product-specific documentation including Certificates of Analysis
- Customer support for technical questions about peptide handling
Research Community:
- Institutional research coordinators for protocol development assistance
- Laboratory safety officers for compliance guidance
- Peer researchers for protocol comparison and optimization strategies
Professional Development:
- Laboratory technique courses emphasizing aseptic procedures
- Research methodology workshops focusing on documentation standards
- Peptide science seminars covering advances in research applications
Final Thoughts on Research Excellence
Mastery of tirzepatide dose in units calculations represents more than technical competence—it reflects commitment to research integrity that distinguishes professional laboratory work from amateur experimentation. Every precisely measured dose, every documented calculation, and every verified administration contributes to the validity of research findings and the advancement of scientific knowledge.
The researchers who achieve the most reliable, reproducible results are those who approach dosing with the same rigor they apply to experimental design and data analysis. They understand that precision in the seemingly mundane task of converting milligrams to units directly impacts the quality of their research outcomes.
By implementing the calculation methods, verification procedures, and documentation standards outlined in this guide, researchers position themselves for success in tirzepatide research protocols. Whether investigating metabolic pathways, optimizing dose-response relationships, or exploring novel applications, accurate unit-based dosing provides the foundation upon which meaningful discoveries are built.
For premium research-grade tirzepatide and comprehensive support throughout your research journey, PEPTIDE PRO delivers the quality, consistency, and professional service that research excellence demands. With high-purity compounds, fast UK delivery, and expert guidance, your research protocols receive the support they deserve.