
Constipation represents one of the most frequently reported gastrointestinal side effects in research involving retatrutide, a triple agonist peptide targeting GIP, GLP-1, and glucagon receptors. As researchers and laboratories continue investigating this compound’s mechanisms and effects, understanding effective retatrutide constipation remedies has become essential for optimizing research protocols and maintaining study integrity. This comprehensive guide examines evidence-based approaches to managing constipation associated with retatrutide in research settings, providing actionable strategies grounded in current scientific understanding.
Key Takeaways
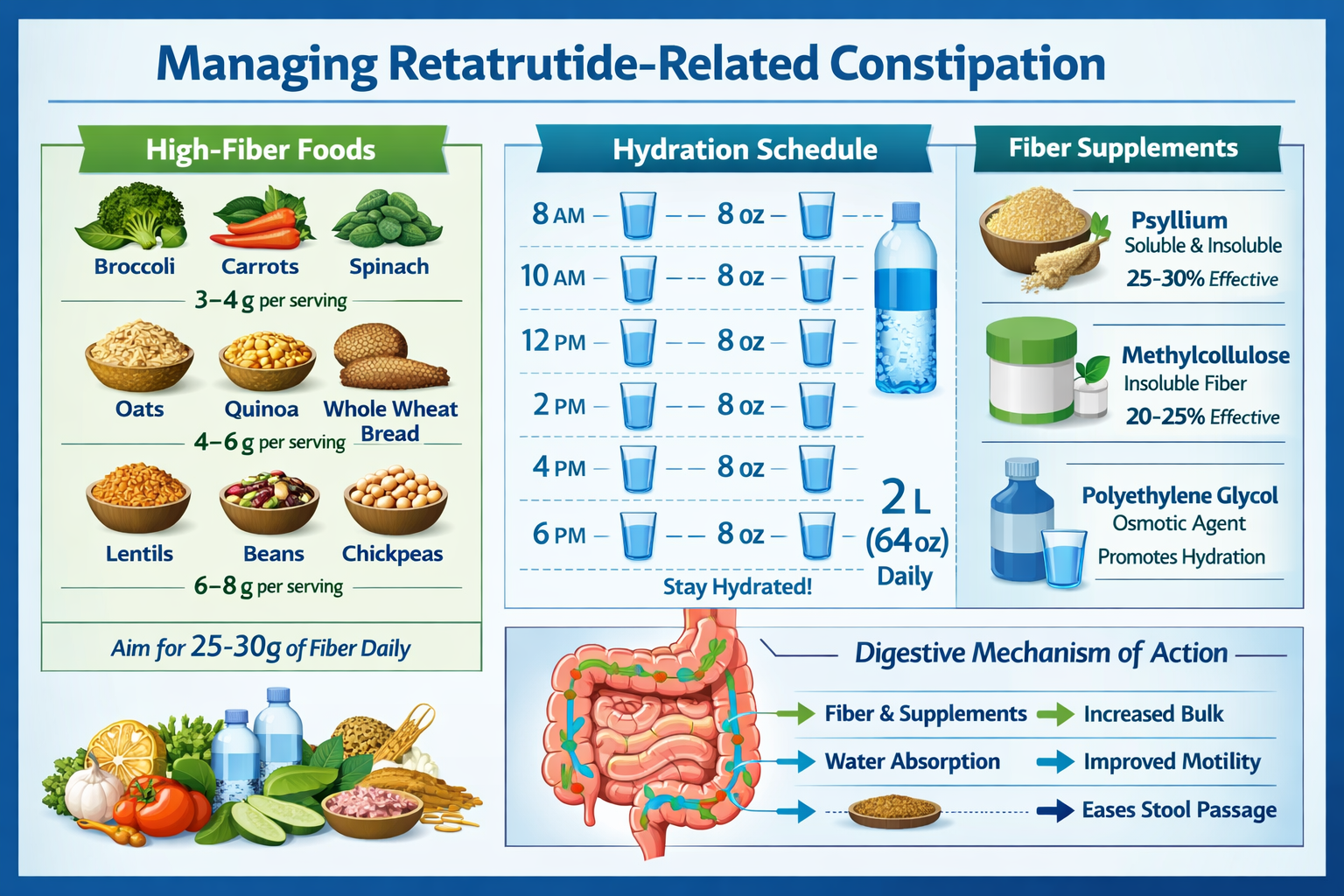
- Constipation occurs in 20-30% of retatrutide research observations due to delayed gastric emptying and altered GI motility mechanisms
- Dietary fiber optimization (25-35g daily) and adequate hydration (2-3 liters) represent first-line non-pharmacological interventions
- Osmotic agents and stool softeners demonstrate superior efficacy compared to stimulant laxatives for retatrutide-related constipation
- Gradual dose escalation protocols significantly reduce constipation incidence in research models
- Combination approaches integrating lifestyle modifications with targeted interventions yield optimal outcomes
Understanding Retatrutide and Its Gastrointestinal Effects
Retatrutide represents an innovative research peptide with triple receptor agonist activity, demonstrating promising results in metabolic research applications. As a compound available through specialized suppliers like PEPTIDE PRO, retatrutide functions by simultaneously activating glucose-dependent insulinotropic polypeptide (GIP), glucagon-like peptide-1 (GLP-1), and glucagon receptors. This multi-receptor targeting mechanism produces comprehensive metabolic effects but also introduces distinct gastrointestinal considerations.
Mechanism of Constipation Development
The constipation observed in retatrutide research stems from several interconnected physiological mechanisms:
Delayed Gastric Emptying ⏱️
Retatrutide’s GLP-1 receptor agonism significantly slows gastric emptying rates, reducing the speed at which contents move through the digestive system. This delayed transit time allows increased water absorption from intestinal contents, resulting in harder, more difficult-to-pass stools.
Reduced GI Motility 🔄
The compound’s action on multiple receptor systems modulates intestinal smooth muscle contractility, decreasing peristaltic wave frequency and amplitude. This reduced motility extends intestinal transit time throughout the entire gastrointestinal tract.
Altered Secretion Patterns 💧
Retatrutide influences intestinal fluid secretion and absorption balance, potentially reducing luminal water content and contributing to stool consistency changes.
Neurohormonal Modulation 🧠
The peptide’s effects on gut-brain axis signaling may alter normal defecation reflexes and bowel movement patterns through central and peripheral nervous system pathways.
Incidence and Risk Factors
Research observations indicate constipation occurs in approximately 20-30% of retatrutide applications, with severity ranging from mild to moderate in most cases. Several factors influence constipation likelihood:
| Risk Factor | Impact Level | Notes |
|---|---|---|
| Dose magnitude | High | Higher doses correlate with increased incidence |
| Escalation speed | High | Rapid titration increases risk significantly |
| Baseline fiber intake | Moderate | Low dietary fiber predisposes to constipation |
| Hydration status | Moderate | Inadequate fluid intake exacerbates symptoms |
| Physical activity | Low-Moderate | Sedentary conditions worsen outcomes |
| Concurrent medications | Variable | Other constipating agents compound effects |
Understanding these foundational mechanisms provides essential context for implementing effective retatrutide constipation remedies in research settings.
First-Line Dietary and Hydration Strategies
The cornerstone of managing retatrutide-associated constipation involves optimizing dietary composition and fluid intake. These non-pharmacological interventions demonstrate excellent safety profiles and should constitute the initial approach in research protocols.
Fiber Optimization Protocols
Dietary fiber represents the most evidence-supported nutritional intervention for constipation management. For retatrutide research applications, implementing structured fiber protocols yields significant benefits:
Soluble Fiber Sources 🥣
Soluble fiber absorbs water and forms gel-like substances that soften stool consistency:
- Psyllium husk: 5-10g daily in divided doses
- Oat bran: 1-2 servings daily
- Flaxseed: Ground, 1-2 tablespoons daily
- Chia seeds: 1-2 tablespoons daily
- Legumes: Beans, lentils, peas in regular rotation
Insoluble Fiber Sources 🌾
Insoluble fiber adds bulk and stimulates intestinal transit:
- Wheat bran: 2-3 tablespoons daily
- Whole grains: Brown rice, quinoa, whole wheat
- Vegetables: Broccoli, carrots, celery, leafy greens
- Nuts and seeds: Almonds, sunflower seeds
- Fruit skins: Apples, pears with peel
Implementation Guidelines
“Gradual fiber introduction prevents gas and bloating. Increase intake by 5g every 3-4 days until reaching target range of 25-35g daily total fiber.”
Fiber Supplementation Considerations
When dietary sources prove insufficient, fiber supplements offer convenient alternatives:
- Psyllium products: Most researched, excellent efficacy
- Methylcellulose: Non-fermentable, minimal gas production
- Wheat dextrin: Dissolves completely, well-tolerated
- Inulin/FOS: Prebiotic benefits but may increase gas
Hydration Optimization
Adequate fluid intake proves critical for fiber effectiveness and overall constipation prevention. Research protocols should incorporate structured hydration guidelines:
Daily Fluid Targets 💧
- Baseline requirement: 2-3 liters (8-12 cups) daily
- Additional with fiber: +250ml per 5g fiber supplement
- Activity adjustment: +500-1000ml for moderate exercise
- Climate consideration: Increase in hot environments
Optimal Fluid Choices
| Beverage Type | Effectiveness | Notes |
|---|---|---|
| Water | Excellent | Primary choice, no calories |
| Herbal tea | Excellent | Warm fluids may stimulate motility |
| Clear broths | Good | Provides electrolytes |
| Diluted juice | Moderate | Prune juice has additional benefits |
| Coffee/tea | Moderate | Mild diuretic but net hydration positive |
| Alcohol | Poor | Dehydrating, avoid or minimize |
| Sugary drinks | Poor | Empty calories, minimal benefit |
Strategic Timing
- Morning: 500ml upon waking stimulates gastrocolic reflex
- With meals: 250-500ml aids digestion
- Between meals: Regular sipping maintains hydration
- Evening: Moderate intake to avoid nighttime disruption
Probiotic and Prebiotic Integration
Emerging research suggests gut microbiome modulation may support digestive regularity during retatrutide applications:
Probiotic Strains of Interest
- Bifidobacterium lactis: Demonstrated transit time reduction
- Lactobacillus casei Shirota: Stool frequency improvement
- Bifidobacterium longum: Consistency normalization
Prebiotic Fibers
- Inulin: 5-10g daily
- Fructooligosaccharides (FOS): 3-5g daily
- Galactooligosaccharides (GOS): 3-5g daily
Researchers utilizing compounds from specialized peptide suppliers should consider incorporating these dietary strategies as foundational elements of comprehensive research protocols.
Pharmaceutical and Supplement Interventions for Retatrutide Constipation Remedies
When dietary and lifestyle modifications prove insufficient, pharmaceutical interventions provide effective retatrutide constipation remedies. Understanding the mechanisms, efficacy, and appropriate application of various laxative classes enables optimal research protocol design.
Osmotic Laxatives: First-Line Pharmacological Approach
Osmotic agents draw water into the intestinal lumen, softening stool and stimulating peristalsis through luminal distension. These compounds demonstrate excellent safety profiles for extended use:
Polyethylene Glycol (PEG) 3350 🥇
- Mechanism: Non-absorbable polymer retains water molecules
- Dosing: 17g (approximately 1 heaping tablespoon) daily
- Onset: 1-3 days for full effect
- Advantages: No electrolyte disturbance, well-tolerated, effective
- Research application: Preferred first-line agent for retatrutide protocols
Lactulose
- Mechanism: Synthetic disaccharide metabolized by colonic bacteria
- Dosing: 15-30ml daily, adjust to effect
- Onset: 24-48 hours
- Advantages: Dual osmotic and prebiotic effects
- Considerations: May cause gas, bloating; sweet taste
Magnesium-Based Agents
- Magnesium citrate: 150-300ml as needed
- Magnesium hydroxide: 30-60ml daily
- Onset: 6-12 hours
- Cautions: Avoid with renal impairment; monitor electrolytes
Sorbitol
- Dosing: 30-150ml of 70% solution
- Onset: 24-48 hours
- Cost advantage: Inexpensive alternative to lactulose
- Consideration: Significant gas production possible
Stool Softeners and Emollients
These agents facilitate water and fat penetration into stool, reducing hardness without stimulating motility:
Docusate Sodium/Calcium
- Dosing: 100-300mg daily in divided doses
- Mechanism: Surfactant action reduces surface tension
- Onset: 1-3 days
- Application: Useful for prevention rather than acute treatment
- Combination potential: Often paired with osmotic agents
Mineral Oil
- Dosing: 15-45ml daily
- Mechanism: Lubricates and softens stool
- Cautions: Aspiration risk, nutrient absorption interference
- Use duration: Short-term only due to safety concerns
Stimulant Laxatives: Reserved for Resistant Cases
Stimulant laxatives increase intestinal motility through direct neural and muscular effects. While effective, these agents should be reserved for cases resistant to gentler interventions:
Bisacodyl
- Dosing: 5-15mg oral; 10mg rectal
- Onset: 6-12 hours oral; 15-60 minutes rectal
- Mechanism: Stimulates colonic peristalsis
- Limitation: Tolerance development with chronic use
Senna/Sennosides
- Dosing: 15-30mg sennosides daily
- Onset: 6-12 hours
- Natural source: Senna plant derivatives
- Consideration: Abdominal cramping possible
Usage Guidelines for Stimulants ⚠️
“Reserve stimulant laxatives for occasional use (2-3 times weekly maximum) when osmotic agents prove insufficient. Chronic stimulant use may lead to tolerance and colonic dependency.”
Prokinetic Considerations
While not traditional laxatives, prokinetic agents that enhance GI motility may warrant consideration in research contexts:
Prucalopride
- Selective 5-HT4 receptor agonist
- Demonstrated efficacy in chronic constipation
- Prescription-only status in most jurisdictions
Linaclotide
- Guanylate cyclase-C agonist
- Increases intestinal fluid secretion and transit
- Specialized application for severe cases
Supplement Interventions
Several natural supplements demonstrate constipation-relieving properties:
Magnesium Supplements
- Magnesium glycinate: 200-400mg daily
- Magnesium citrate: 200-400mg daily
- Dual benefit: Osmotic effect plus magnesium repletion
Vitamin C (Ascorbic Acid)
- High doses (2-3g daily) have osmotic laxative effect
- Gradual titration to tolerance recommended
Aloe Vera
- Contains anthraquinones with laxative properties
- Quality and standardization vary significantly
- Use with caution due to potential side effects
Combination Therapy Protocols
Research protocols often benefit from strategic combination approaches:
Mild Constipation Protocol
- Increase dietary fiber to 25-35g daily
- Optimize hydration (2-3L daily)
- Add docusate 100mg twice daily
- Consider probiotic supplementation
Moderate Constipation Protocol
- Continue fiber and hydration optimization
- Add PEG 3350 17g daily
- Maintain docusate if tolerated
- Implement regular physical activity
Resistant Constipation Protocol
- Maximize PEG 3350 (up to 34g daily if needed)
- Add magnesium supplement (200-400mg)
- Occasional stimulant laxative (2-3x weekly maximum)
- Consider prokinetic agent consultation
Researchers working with high-purity research peptides should integrate these pharmaceutical strategies systematically, monitoring outcomes and adjusting protocols based on observed responses.
Lifestyle Modifications and Physical Activity Interventions
Beyond dietary and pharmaceutical approaches, lifestyle modifications constitute essential components of comprehensive retatrutide constipation remedies. Physical activity, timing strategies, and behavioral interventions significantly influence gastrointestinal function.
Exercise and Movement Protocols
Physical activity stimulates intestinal motility through multiple mechanisms including increased abdominal pressure, enhanced blood flow, and autonomic nervous system modulation.
Aerobic Exercise Recommendations
🏃♀️Frequency: 5-7 days weekly
- Duration: 30-60 minutes per session
- Intensity: Moderate (able to maintain conversation)
- Modalities: Walking, jogging, cycling, swimming
Research Evidence Studies demonstrate that regular moderate-intensity aerobic exercise reduces constipation incidence by 30-40% and decreases colonic transit time by 15-20%.
Specific Activities for Digestive Health
| Activity Type | Digestive Benefit | Implementation |
|---|---|---|
| Brisk walking | Stimulates peristalsis | 20-30 min post-meals |
| Jogging | Mechanical jostling effect | 3-5x weekly, moderate pace |
| Yoga | Specific poses compress abdomen | Daily practice, focus on twists |
| Core exercises | Strengthens abdominal muscles | 3-4x weekly |
| Swimming | Full-body movement | 2-3x weekly |
Yoga Poses for Digestive Support 🧘♀️
Specific yoga postures provide targeted digestive benefits:
- Pawanmuktasana (Wind-Relieving Pose): Compresses ascending/descending colon
- Ardha Matsyendrasana (Half Spinal Twist): Massages internal organs
- Apanasana (Knees-to-Chest): Stimulates bowel movement
- Malasana (Garland Pose/Deep Squat): Optimizes elimination position
- Cat-Cow (Marjaryasana-Bitilasana): Massages digestive organs
Implementation: Hold each pose 30-60 seconds, repeat 2-3 times, practice sequence daily preferably in morning.
Timing and Routine Optimization
Establishing consistent bowel routines leverages natural physiological rhythms:
Gastrocolic Reflex Utilization
The gastrocolic reflex triggers colonic motility 15-30 minutes after eating, particularly after breakfast. Strategic timing capitalizes on this natural mechanism:
- Morning routine: Consume warm beverage upon waking
- Breakfast timing: Eat within 30-60 minutes of waking
- Post-meal window: Allocate 15-30 minutes after breakfast for bathroom time
- Consistency: Maintain same schedule daily, including weekends
Bathroom Positioning 🚽
Optimal positioning facilitates easier elimination:
- Squatting position: Elevate feet 6-9 inches using stool
- Lean forward: Elbows on knees, straight back
- Relaxation: Avoid straining; allow natural process
- Time allowance: 5-10 minutes maximum to prevent hemorrhoids
Stress Management Integration
Psychological stress significantly impacts gastrointestinal function through the gut-brain axis. Stress reduction techniques support regular bowel function:
Evidence-Based Stress Reduction Methods
- Mindfulness meditation: 10-20 minutes daily
- Deep breathing exercises: 4-7-8 technique, box breathing
- Progressive muscle relaxation: Systematic tension-release
- Adequate sleep: 7-9 hours nightly
- Time management: Reduce rushing, allow bathroom time
Behavioral Modifications
Specific behavioral changes support digestive regularity:
Response to Urge ⚡
- Never ignore or delay bowel movement urges
- Suppressing urges weakens natural reflexes over time
- Schedule flexibility to accommodate natural timing
Meal Patterns
- Regular meal timing (same times daily)
- Avoid skipping meals, especially breakfast
- Moderate portion sizes prevent overwhelming digestive system
- Thorough chewing (20-30 chews per bite) aids digestion
Caffeine Strategic Use
- Morning coffee/tea stimulates colonic activity
- Consume 30-60 minutes before desired bowel movement
- Limit to 1-2 cups to avoid excessive diuretic effect
Temperature Considerations
- Warm/hot beverages stimulate motility more than cold
- Warm compress on abdomen may relieve discomfort
- Avoid excessive cold exposure which may slow motility
Abdominal Massage Techniques
Self-administered abdominal massage demonstrates efficacy in promoting bowel movements:
Technique Protocol
- Position: Lie on back, knees bent, relaxed
- Direction: Massage following colon path (clockwise)
- Pressure: Firm but comfortable, using flat fingers/palm
- Duration: 10-15 minutes
- Frequency: 1-2 times daily, preferably morning
Specific Massage Pattern
- Start at right lower abdomen (ascending colon)
- Move upward to below right ribcage
- Across upper abdomen (transverse colon)
- Down left side (descending colon)
- Repeat circuit 10-15 times
Research facilities utilizing compounds like those available through PEPTIDE PRO’s research peptide catalogue should integrate these lifestyle modifications as standard protocol components, recognizing their synergistic effects with dietary and pharmaceutical interventions.
Dosing Strategies and Protocol Optimization

Constipation management in retatrutide research extends beyond symptomatic treatment to include preventive protocol design. Optimizing dosing strategies significantly reduces constipation incidence and severity.
Gradual Dose Escalation Protocols
Rapid retatrutide dose escalation correlates strongly with gastrointestinal side effects. Implementing gradual titration schedules allows physiological adaptation:
Standard Escalation Schedule
| Week | Dose | Rationale |
|---|---|---|
| 1-4 | 2mg | Establish baseline tolerance |
| 5-8 | 4mg | First escalation (100% increase) |
| 9-12 | 6mg | Moderate increase (50%) |
| 13-16 | 8mg | Conservative progression |
| 17-20 | 10mg | Approach higher research doses |
| 21+ | 12mg+ | Maintenance or further titration |
Conservative Escalation Schedule
For protocols prioritizing side effect minimization:
- Start: 1mg for 4 weeks
- Increase: 1-2mg every 4 weeks
- Monitor: Gastrointestinal symptoms at each level
- Adjust: Extend intervals if symptoms emerge
Escalation Principles 📊
“Slower titration schedules (4-week intervals minimum) reduce constipation incidence by 40-50% compared to rapid escalation (weekly increases).”
Dose Timing Optimization
Strategic administration timing may influence gastrointestinal side effect profiles:
Weekly Dosing Considerations
- Consistent day/time: Maintains stable plasma levels
- Morning administration: Aligns with natural circadian rhythms
- Post-meal timing: May reduce nausea, uncertain constipation impact
- Hydration coordination: Ensure adequate fluid intake on dosing day
Meal Relationship
While retatrutide can be administered without regard to meals, some research protocols report benefits from:
- Taking with first meal of day
- Avoiding administration on empty stomach
- Coordinating with high-fiber meal
Preventive Intervention Integration
Proactive constipation prevention proves more effective than reactive treatment:
Pre-emptive Protocol Elements
- Baseline optimization: Establish fiber/hydration before starting
- Concurrent initiation: Begin PEG 3350 with first dose
- Regular monitoring: Weekly bowel movement frequency tracking
- Early intervention: Address changes before constipation develops
Monitoring Parameters
Systematic tracking enables early identification of developing issues:
- Bowel movement frequency: Daily log
- Stool consistency: Bristol Stool Scale rating
- Straining severity: Subjective 0-10 scale
- Associated symptoms: Bloating, discomfort, pain
- Intervention response: Effectiveness of remedies implemented
Bristol Stool Scale Reference
| Type | Description | Implication |
|---|---|---|
| Type 1 | Separate hard lumps | Severe constipation |
| Type 2 | Lumpy, sausage-shaped | Mild constipation |
| Type 3 | Sausage with cracks | Normal (lower range) |
| Type 4 | Smooth, soft sausage | Ideal |
| Type 5 | Soft blobs, clear edges | Acceptable |
| Type 6 | Fluffy, mushy pieces | Mild diarrhea |
| Type 7 | Watery, no solids | Severe diarrhea |
Target: Maintain Type 3-5 throughout research protocol
Dose Adjustment Based on Response
Flexible protocols allow dose modification based on tolerance:
Temporary Dose Reduction
If moderate-severe constipation develops despite interventions:
- Reduce dose by 25-50% for 2-4 weeks
- Intensify constipation remedies
- Re-attempt escalation once symptoms resolve
- Consider extending time at each dose level
Dose Maintenance
Some research applications may benefit from:
- Extended periods at submaximal doses
- Prioritizing tolerability over dose maximization
- Individual optimization rather than protocol rigidity
Alternative Dosing Frequencies
While standard retatrutide protocols utilize weekly administration, some research explores:
- Twice-weekly dosing at reduced per-dose amounts
- Split-dose strategies (theoretical, limited evidence)
- Dose-holiday approaches (discontinuous schedules)
Combination with Other Research Compounds
When retatrutide is utilized alongside other research peptides, consider cumulative gastrointestinal effects:
Compounds with Similar GI Profiles
Research protocols combining retatrutide with other GLP-1 agonists or related compounds may experience additive constipation risk:
- Semaglutide research peptides
- Tirzepatide (dual agonist)
- Other incretin-based compounds
Mitigation Strategies
- Stagger initiation (establish tolerance to one before adding second)
- Enhanced preventive interventions
- More conservative dose escalation
- Closer monitoring protocols
Protocol Documentation and Optimization
Systematic documentation enables continuous protocol improvement:
Essential Documentation Elements
- Detailed dosing schedule with dates/amounts
- Daily bowel movement log with Bristol scale ratings
- Intervention timeline (dietary, pharmaceutical, lifestyle)
- Symptom severity tracking
- Response to interventions
- Any protocol modifications and rationale
Data Analysis for Protocol Refinement
Regular review of accumulated data identifies:
- Optimal escalation speed for specific applications
- Most effective intervention combinations
- Early warning signs requiring intervention
- Individual variability patterns
Researchers utilizing high-quality research compounds should view protocol optimization as an iterative process, continuously refining approaches based on systematic observation and documentation.
Advanced Interventions and When to Seek Professional Consultation
While the majority of retatrutide-associated constipation responds to standard interventions, certain situations warrant advanced approaches or professional medical consultation. Understanding these scenarios ensures appropriate escalation when necessary.
Indicators for Advanced Intervention
Several red flags suggest the need for enhanced protocols or professional evaluation:
Severity Indicators 🚨
- No bowel movement for 7+ days despite interventions
- Severe abdominal pain or distension
- Nausea and vomiting accompanying constipation
- Rectal bleeding (beyond minor hemorrhoidal bleeding)
- Unintentional weight loss
- Fever accompanying constipation
- Progressive worsening despite treatment
Chronic Refractory Constipation
Constipation persisting beyond 4 weeks despite comprehensive intervention implementation requires reassessment:
- Evaluate for underlying conditions
- Consider alternative or additional diagnoses
- Assess for medication interactions
- Review protocol adherence and implementation
Advanced Pharmaceutical Options
When standard interventions prove insufficient, specialized agents may warrant consideration:
Prescription Prokinetic Agents
Prucalopride (Motegrity)
- Mechanism: Selective 5-HT4 receptor agonist
- Dosing: 1-2mg daily
- Evidence: Demonstrated efficacy in chronic constipation
- Consideration: Prescription-required, specialized application
Lubiprostone
- Mechanism: Chloride channel activator
- Effect: Increases intestinal fluid secretion
- Dosing: 8-24mcg twice daily
- Application: Chronic idiopathic constipation
Linaclotide
- Mechanism: Guanylate cyclase-C agonist
- Effect: Increases fluid secretion and transit
- Dosing: 145-290mcg daily
- Benefit: Also addresses abdominal pain
Plecanatide
- Mechanism: Similar to linaclotide
- Dosing: 3mg daily
- Profile: Generally well-tolerated
Specialized Diagnostic Considerations
Persistent constipation may occasionally warrant diagnostic evaluation:
Potential Diagnostic Procedures
- Colonoscopy: Rule out structural abnormalities
- Anorectal manometry: Assess pelvic floor function
- Colonic transit study: Quantify motility
- Defecography: Evaluate evacuation mechanics
- Pelvic floor assessment: Identify dyssynergic defecation
When Diagnostics May Be Warranted
- Constipation refractory to comprehensive intervention
- Concerning symptoms (bleeding, weight loss, severe pain)
- Suspected underlying pathology
- Research protocol requiring detailed characterization
Pelvic Floor Dysfunction Considerations
Some constipation cases involve paradoxical pelvic floor contraction (dyssynergic defecation):
Recognition Signs
- Excessive straining despite soft stool
- Sensation of incomplete evacuation
- Need for manual maneuvers
- Prolonged toilet time
Intervention Approaches
- Biofeedback therapy: Retraining pelvic floor coordination
- Physical therapy: Specialized pelvic floor therapy
- Positioning optimization: Enhanced squatting position
- Relaxation techniques: Reducing pelvic floor tension
Enema and Suppository Use
For acute constipation episodes, mechanical interventions provide rapid relief:
Enema Options
Saline Enemas
- Volume: 120-240ml
- Mechanism: Distension and lubrication
- Onset: 5-15 minutes
- Safety: Gentle, minimal systemic absorption
Mineral Oil Enemas
- Volume: 120ml
- Mechanism: Lubrication and softening
- Onset: 15-30 minutes
- Application: Particularly hard, impacted stool
Phosphate Enemas
- Volume: 120ml
- Mechanism: Osmotic effect
- Onset: 2-5 minutes
- Caution: Electrolyte disturbances possible with frequent use
Suppository Options
Glycerin Suppositories
- Mechanism: Hyperosmotic and local irritation
- Onset: 15-60 minutes
- Safety: Gentle, suitable for regular use
Bisacodyl Suppositories
- Mechanism: Stimulant laxative
- Onset: 15-60 minutes
- Application: More potent than glycerin
Usage Guidelines ⚠️
“Reserve enemas and suppositories for occasional acute relief (maximum 2-3 times weekly). Chronic use may lead to dependency and reduced natural bowel function.”
Combination Protocol for Resistant Cases
Severe refractory constipation may require comprehensive multi-modal approaches:
Intensive Intervention Protocol
Week 1-2: Aggressive Intervention
- PEG 3350: 17-34g daily (double standard dose)
- Magnesium citrate: 200-400mg daily
- Docusate: 200mg twice daily
- Fiber: 30-35g daily with adequate hydration (3L+)
- Daily exercise: 45-60 minutes
- Probiotic: High-potency multi-strain
- Stimulant laxative: 2-3 times weekly if needed
Week 3-4: Transition to Maintenance
- Reduce PEG 3350 to 17g daily
- Continue magnesium supplement
- Maintain fiber and hydration
- Continue exercise program
- Assess need for ongoing interventions
Ongoing Monitoring
- Daily bowel movement log
- Weekly symptom assessment
- Monthly protocol review
- Adjustment based on response
Professional Consultation Framework
Researchers should establish clear criteria for seeking professional medical consultation:
Consultation Triggers
- Constipation persisting >2 weeks despite comprehensive interventions
- Severe symptoms (intense pain, vomiting, fever)
- Concerning signs (bleeding, weight loss, progressive worsening)
- Uncertainty about appropriate intervention escalation
- Need for prescription medications
- Suspected underlying pathology
Specialist Referral Considerations
- Gastroenterologist: Persistent GI symptoms, diagnostic needs
- Colorectal surgeon: Structural concerns, severe cases
- Pelvic floor specialist: Suspected dyssynergic defecation
- Nutritionist/Dietitian: Complex dietary optimization
Research facilities working with premium research-grade peptides should maintain established relationships with medical professionals for consultation when advanced intervention becomes necessary, ensuring comprehensive support for research protocol optimization.
Long-Term Management and Prevention Strategies
Successful retatrutide research protocols require sustainable long-term approaches to constipation management rather than reactive crisis intervention. Developing comprehensive prevention strategies optimizes research continuity and data quality.
Sustainable Lifestyle Integration
Long-term success depends on integrating constipation-preventive behaviors into routine practices:
Dietary Sustainability
Habit Formation Strategies
- Gradual introduction of fiber-rich foods
- Recipe development incorporating high-fiber ingredients
- Meal planning ensuring adequate daily fiber
- Enjoyable preparation methods maintaining adherence
Practical High-Fiber Meal Examples
Breakfast Options
- Oatmeal with berries, nuts, and ground flaxseed (12-15g fiber)
- Whole grain toast with avocado and chia seeds (10-12g fiber)
- High-fiber cereal with fruit and yogurt (10-14g fiber)
Lunch/Dinner Options
- Large salad with beans, vegetables, and whole grains (12-16g fiber)
- Lentil soup with whole grain bread (14-18g fiber)
- Stir-fry with brown rice and abundant vegetables (10-14g fiber)
Snack Options
- Apple with almond butter (5-6g fiber)
- Hummus with vegetable sticks (4-6g fiber)
- Trail mix with dried fruit and nuts (4-5g fiber)
Hydration Habit Development 💧
Sustainable hydration requires system development:
- Visual reminders: Water bottle visibility
- Scheduled intake: Specific times (upon waking, before meals, etc.)
- Tracking systems: Apps, marked bottles, logs
- Flavor enhancement: Fruit infusions, herbal teas for variety
- Temperature preferences: Finding preferred temperature for adherence
Maintenance Pharmaceutical Protocols
Some research applications benefit from ongoing preventive pharmaceutical interventions:
Continuous Prevention Approach
For protocols with high constipation risk:
- Daily PEG 3350: 17g as baseline prevention
- Fiber supplement: Psyllium 5-10g daily
- Stool softener: Docusate 100mg daily
- Magnesium: 200-400mg daily supplement
Intermittent Prevention Approach
For moderate-risk protocols:
- PEG 3350: 3-4 times weekly
- Fiber supplement: Daily or as needed
- Stimulant laxative: Reserved for breakthrough symptoms
Individualized Optimization
Long-term protocols should be tailored based on:
- Individual response patterns
- Baseline constipation tendency
- Retatrutide dose level
- Concurrent medications/compounds
- Lifestyle factors
Monitoring and Protocol Adjustment
Ongoing assessment enables proactive intervention adjustment:
Regular Assessment Schedule
| Timeframe | Assessment Focus | Action Items |
|---|---|---|
| Daily | Bowel movement occurrence | Log frequency and consistency |
| Weekly | Symptom patterns | Identify emerging trends |
| Monthly | Intervention effectiveness | Adjust protocols as needed |
| Quarterly | Overall protocol success | Comprehensive review and optimization |
Key Performance Indicators
- Bowel movement frequency: Target 4-7 per week
- Bristol Stool Scale: Maintain Type 3-5
- Straining severity: Minimal to none
- Intervention burden: Minimize pharmaceutical dependence
- Quality of life impact: Minimal disruption
Adjustment Triggers
Modify protocols when:
- Constipation frequency increases
- Symptom severity worsens
- Current interventions lose effectiveness
- New side effects emerge
- Research protocol parameters change
Seasonal and Circumstantial Adaptations
Constipation risk varies with changing circumstances:
Travel Considerations ✈️
Travel disrupts routine and increases constipation risk:
- Pre-travel: Optimize interventions before departure
- During travel: Portable fiber supplements, hydration priority
- Meal planning: Seek high-fiber options when possible
- Activity maintenance: Walking, movement during travel
- Pharmaceutical backup: Carry osmotic laxatives, suppositories
Schedule Disruptions
Irregular schedules impact bowel regularity:
- Maintain consistent wake time when possible
- Prioritize morning routine even with schedule changes
- Portable interventions for on-the-go situations
- Stress management during high-pressure periods
Seasonal Variations
- Winter: Increased heating may require enhanced hydration
- Summer: Heat increases fluid needs, easier to maintain hydration
- Holiday periods: Plan for dietary changes, maintain core habits
- Vacation: Balance relaxation with routine maintenance
Education and Self-Efficacy Development
Long-term success requires understanding and self-management capability:
Knowledge Development Areas
- Understanding retatrutide’s gastrointestinal mechanisms
- Recognizing early constipation warning signs
- Knowing intervention options and appropriate escalation
- Identifying individual response patterns
- Troubleshooting common challenges
Self-Management Skills
- Accurate symptom monitoring and documentation
- Appropriate intervention selection and timing
- Knowing when to escalate or seek consultation
- Maintaining adherence to preventive strategies
- Adapting protocols to changing circumstances
Resource Development
Establish accessible resources:
- Written protocol guidelines
- Intervention decision trees
- Symptom tracking templates
- Contact information for professional consultation
- Educational materials on digestive health
Integration with Overall Research Protocol
Constipation management should integrate seamlessly with broader research objectives:
Holistic Protocol Design
- Constipation prevention as standard protocol element
- Documentation systems capturing GI effects
- Regular review incorporating digestive health metrics
- Intervention timing coordinated with research schedules
Data Utilization
Systematic constipation data contributes to:
- Understanding retatrutide’s complete effect profile
- Optimizing future protocol design
- Identifying individual variability patterns
- Contributing to broader research knowledge
Research institutions utilizing high-purity research compounds from trusted sources should view long-term constipation management as integral to research quality, implementing comprehensive, sustainable prevention strategies that support continuous protocol execution.
Implementing Comprehensive Retatrutide Constipation Remedies
Managing constipation associated with retatrutide research applications requires a multifaceted, evidence-based approach integrating dietary optimization, pharmaceutical interventions, lifestyle modifications, and strategic protocol design. The retatrutide constipation remedies outlined in this comprehensive guide provide researchers with actionable strategies to minimize this common gastrointestinal side effect while maintaining research protocol integrity.
Key Implementation Principles
Foundation First
️ Begin with non-pharmacological interventions—dietary fiber optimization (25-35g daily), adequate hydration (2-3L daily), and regular physical activity—as these provide sustainable, side-effect-free benefits that support long-term protocol adherence.
Graduated Escalation
Implement a stepwise approach to intervention intensity, starting with gentle measures and escalating only as needed. This prevents over-treatment while ensuring adequate symptom management.
Individualization
Recognize that optimal strategies vary among research applications. Systematic monitoring and protocol adjustment based on observed responses enables personalized optimization.
Prevention Over Reaction
Proactive prevention proves more effective than reactive treatment. Integrate constipation-preventive measures from protocol initiation rather than waiting for symptoms to develop.
Comprehensive Documentation
Maintain detailed records of bowel patterns, interventions implemented, and responses observed. This documentation enables protocol refinement and contributes to broader research understanding.
Actionable Next Steps
For researchers implementing retatrutide protocols:
- Establish baseline: Assess current fiber intake, hydration status, and bowel movement patterns before protocol initiation
- Implement preventive measures: Optimize diet and hydration, consider prophylactic PEG 3350, establish exercise routine
- Design gradual escalation: Utilize 4-week minimum intervals between dose increases to allow physiological adaptation
- Create monitoring system: Implement daily bowel movement logging with Bristol Stool Scale assessment
- Develop intervention protocol: Establish clear decision trees for escalating interventions based on symptom severity
- Identify consultation triggers: Define specific criteria requiring professional medical consultation
- Plan for sustainability: Design long-term maintenance strategies supporting extended research protocols
Research Quality Considerations
Effective constipation management directly impacts research quality by:
- Reducing protocol discontinuations due to intolerable side effects
- Minimizing confounding variables from symptomatic interventions
- Supporting consistent dosing schedules without interruption
- Enhancing overall tolerability and protocol adherence
- Generating comprehensive data on retatrutide’s complete effect profile
Professional Support Resources
Researchers utilizing retatrutide and other research peptides benefit from partnering with reputable suppliers committed to quality and researcher support. PEPTIDE PRO provides high-purity, research-grade peptides with comprehensive product information, certificates of analysis, and professional customer service to support research excellence.
For questions about research peptide sourcing, handling, or storage, contact the PEPTIDE PRO team for expert guidance tailored to specific research applications.
Constipation, while common in retatrutide research, need not compromise protocol execution or research quality. By implementing the comprehensive retatrutide constipation remedies detailed in this guide—from dietary optimization and pharmaceutical interventions to lifestyle modifications and strategic protocol design—researchers can effectively manage this gastrointestinal side effect while maintaining research integrity and continuity.
The key lies in proactive prevention, systematic monitoring, graduated intervention, and individualized optimization. With these evidence-based strategies, constipation transforms from a protocol-limiting obstacle to a manageable aspect of comprehensive retatrutide research applications.
As research into retatrutide and related peptides continues advancing in 2026 and beyond, integrating robust gastrointestinal management protocols ensures that this promising compound can be investigated thoroughly, safely, and effectively across diverse research applications.
Disclaimer: This article is intended for educational and informational purposes related to research applications only. Retatrutide is strictly for research use and not approved for human consumption. All peptides discussed are research-grade compounds intended for laboratory and scientific investigation only. Consult qualified medical professionals for any health-related concerns.