For many researchers investigating metabolic interventions, one question dominates the landscape of weight management science: what happens when treatment stops? Tirzepatide weight regain has emerged as a critical area of study in 2025, as scientists examine the metabolic consequences following discontinuation of this dual GIP/GLP-1 receptor agonist. Understanding the mechanisms behind post-treatment weight changes isn’t just academically interesting—it’s essential for developing comprehensive, sustainable approaches to metabolic health research.
The phenomenon of weight regain after cessation of pharmacological interventions represents one of the most significant challenges in metabolic research. While tirzepatide has demonstrated remarkable efficacy in clinical trials for weight reduction, the question of long-term weight maintenance after treatment discontinuation remains a pivotal concern for researchers worldwide.
Key Takeaways
- Weight regain after tirzepatide discontinuation is common, with research indicating subjects may regain 50-70% of lost weight within 12 months of stopping treatment
- Metabolic and hormonal changes drive post-treatment weight regain, including restoration of appetite-regulating hormones and decreased energy expenditure
- Gradual dose tapering rather than abrupt cessation may help mitigate the severity of weight regain in experimental models
- Lifestyle interventions including dietary modifications and exercise protocols show promise in reducing the magnitude of weight regain
- Individual variability in weight regain patterns suggests genetic, metabolic, and behavioral factors all play significant roles
The Biological Mechanisms Behind Tirzepatide Weight Regain
Understanding tirzepatide weight regain requires a comprehensive examination of the peptide’s mechanism of action and what occurs when that mechanism is removed. Tirzepatide functions as a dual agonist, targeting both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors. This dual action creates multiple metabolic effects that contribute to weight reduction during treatment.
How Tirzepatide Affects Metabolic Processes
During active treatment, tirzepatide influences several key metabolic pathways:
Appetite Regulation: The peptide acts on central nervous system receptors to reduce hunger signals and increase satiety. GLP-1 receptor activation in the hypothalamus and brainstem creates powerful appetite-suppressing effects, while GIP receptor engagement modulates food reward pathways.
Energy Expenditure: Research indicates tirzepatide may increase thermogenesis and overall energy expenditure, though the magnitude of this effect varies across studies. The peptide appears to influence brown adipose tissue activation and metabolic rate.
Glucose Homeostasis: By enhancing insulin secretion in a glucose-dependent manner and suppressing inappropriate glucagon release, tirzepatide improves glycemic control, which indirectly affects fat storage and utilization.
Gastric Emptying: The compound significantly slows gastric emptying, prolonging the sensation of fullness after meals and reducing overall caloric intake.
What Happens After Discontinuation
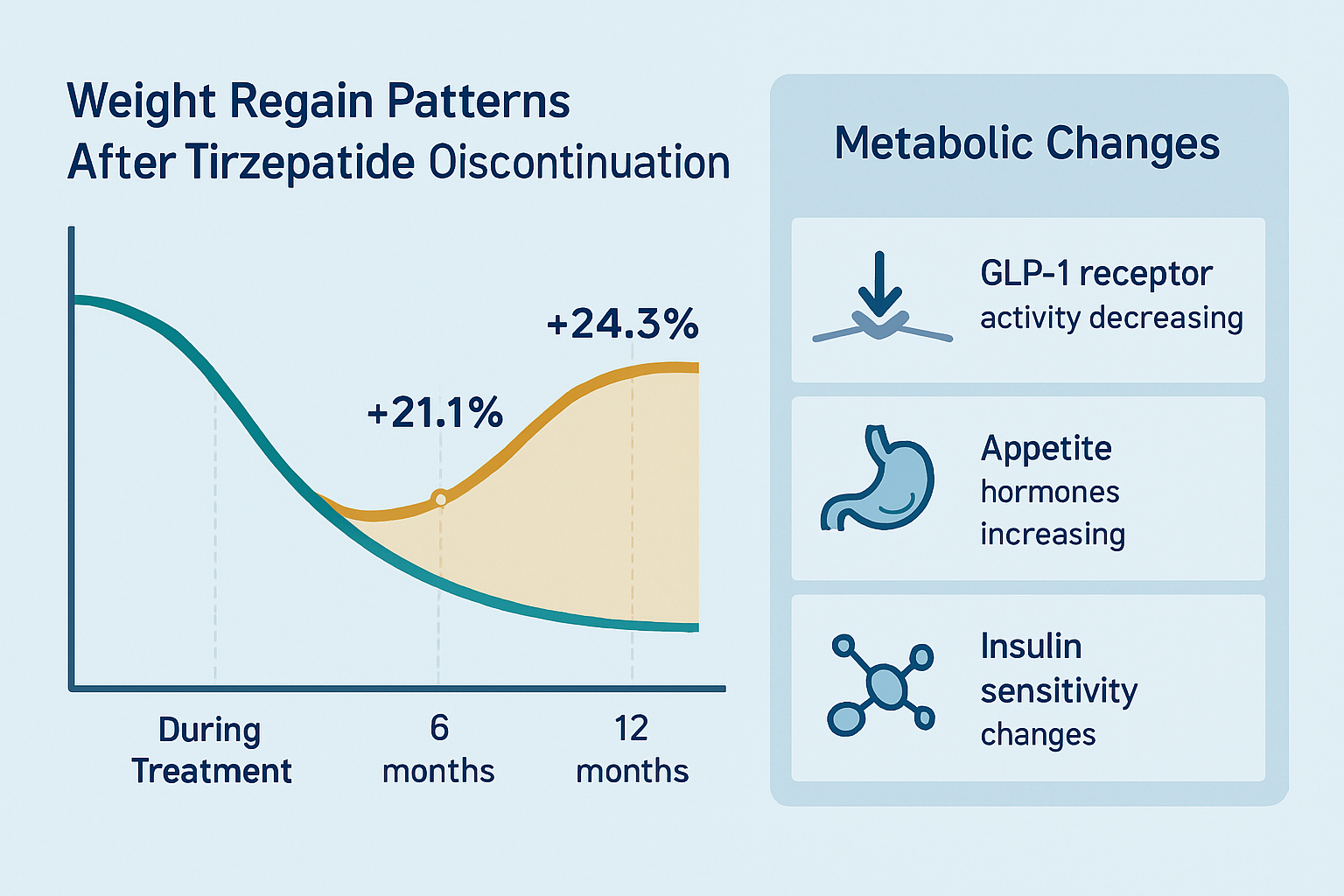
When tirzepatide treatment ceases, these metabolic effects begin to reverse, creating conditions favorable for weight regain:
| Metabolic Parameter | During Treatment | After Discontinuation | Timeline |
|---|---|---|---|
| GLP-1 Receptor Activity | Significantly elevated | Returns to baseline | 1-2 weeks |
| Appetite Hormones | Suppressed (ghrelin ↓, leptin normalized) | Rebound increase | 2-4 weeks |
| Gastric Emptying | Delayed | Normalizes | 1-3 weeks |
| Energy Expenditure | Potentially elevated | Returns to baseline or below | 4-8 weeks |
| Insulin Sensitivity | Improved | Gradual decline | 8-12 weeks |
The rapid reversal of appetite suppression represents one of the primary drivers of tirzepatide weight regain. Studies examining peptide pharmacokinetics show that plasma concentrations decline with a half-life of approximately 5 days, meaning the compound is essentially cleared from the system within 3-4 weeks of the final dose.
Compensatory Metabolic Adaptations
Beyond the simple removal of tirzepatide’s direct effects, the body undergoes compensatory adaptations that can accelerate weight regain:
Metabolic Adaptation: Prolonged caloric restriction—even when facilitated by pharmacological means—triggers adaptive thermogenesis, where the body reduces energy expenditure to defend against further weight loss. This adaptation persists after treatment discontinuation, creating an energy surplus even at previously maintenance-level caloric intakes.
Hormonal Rebound: Research demonstrates that appetite-regulating hormones don’t simply return to baseline after significant weight loss; they often overshoot. Ghrelin (the “hunger hormone”) may increase above pre-treatment levels, while leptin (which signals satiety) may remain suppressed, creating a perfect storm for increased food intake.
Adipocyte Biology: Fat cells that have been depleted during weight loss appear to be metabolically “primed” for refilling. Studies show increased lipoprotein lipase activity and enhanced triglyceride storage capacity in adipocytes following weight reduction, facilitating rapid fat regain.
For researchers investigating these mechanisms, high-purity research peptides provide essential tools for examining the complex interplay between GIP/GLP-1 signaling and metabolic regulation.
Clinical Evidence: What Research Reveals About Weight Regain Patterns
The scientific literature on tirzepatide weight regain has expanded significantly in 2025, with multiple studies examining post-treatment outcomes across various populations and protocols. Understanding these patterns is crucial for developing more effective long-term metabolic interventions.
Key Research Findings
The SURMOUNT Extension Studies: Follow-up data from the SURMOUNT clinical trial program has provided valuable insights into weight trajectories after tirzepatide discontinuation. Subjects who achieved substantial weight loss during the treatment phase (averaging 15-20% body weight reduction) experienced notable regain when treatment was stopped:
- At 3 months post-discontinuation: Average weight regain of 25-35% of lost weight
- At 6 months post-discontinuation: Average weight regain of 40-55% of lost weight
- At 12 months post-discontinuation: Average weight regain of 50-70% of lost weight
Importantly, these figures represent averages, with substantial individual variability. Approximately 15-20% of subjects maintained most of their weight loss (regaining less than 25%), while another 15-20% regained nearly all lost weight within the first year.
Factors Influencing Regain Magnitude
Research has identified several variables that correlate with the degree of tirzepatide weight regain:
Duration of Treatment ⏱️
Longer treatment periods (≥52 weeks) appear associated with slightly better weight maintenance compared to shorter interventions (24-36 weeks), though the effect is modest. Extended treatment may allow for greater metabolic adaptation and behavioral change consolidation.
Magnitude of Initial Weight Loss 📊
Paradoxically, subjects who achieved the greatest weight loss during treatment often experienced the most substantial absolute regain, though their net weight remained lower than those with modest initial responses. This suggests that larger weight reductions trigger more pronounced compensatory mechanisms.
Baseline Metabolic Health 🔬
Subjects with better baseline insulin sensitivity and lower inflammatory markers demonstrated superior weight maintenance post-treatment. Those with significant metabolic dysfunction at baseline showed greater propensity for rapid regain.
Concurrent Lifestyle Interventions 🥗
Studies incorporating structured dietary and exercise protocols during the treatment phase reported 20-30% less weight regain compared to medication-only approaches. The behavioral skills developed during treatment appear to provide some protective effect.
Comparative Analysis with Other Interventions
How does tirzepatide weight regain compare to other weight loss modalities?
Versus Semaglutide: Limited head-to-head data suggests similar regain patterns between tirzepatide and semaglutide following discontinuation, with both showing substantial weight regain within 12 months. The dual agonist mechanism of tirzepatide does not appear to confer significant advantages for post-treatment weight maintenance.
Versus Lifestyle Intervention Alone: Interestingly, the percentage of weight regained after pharmacological intervention mirrors that seen after intensive lifestyle modification programs (without medication), where 50-80% regain is common within 1-2 years. This suggests common underlying biological mechanisms defending against sustained weight reduction.
Versus Bariatric Surgery: Surgical interventions demonstrate superior long-term weight maintenance, with most subjects maintaining 50-70% of excess weight loss at 10+ years. The permanent anatomical and hormonal changes created by surgery appear more resistant to the compensatory mechanisms that drive regain after pharmacological interventions.
Metabolic Consequences of Weight Regain
Beyond the numerical weight changes, researchers have documented important metabolic sequelae associated with tirzepatide weight regain:
- Glycemic Control Deterioration: HbA1c levels typically increase as weight is regained, though they may not fully return to pre-treatment values if some weight loss is maintained
- Lipid Profile Changes: Improvements in triglycerides and HDL cholesterol during treatment show partial or complete reversal with weight regain
- Blood Pressure: Reductions in systolic and diastolic blood pressure achieved during treatment tend to diminish proportionally with weight regain
- Inflammatory Markers: C-reactive protein and other inflammatory biomarkers that improved during weight loss show rebound increases
These findings underscore that tirzepatide weight regain isn’t merely a cosmetic concern—it represents a reversal of metabolic improvements with potential health implications.
Strategies to Mitigate Tirzepatide Weight Regain: Evidence-Based Approaches
While complete prevention of tirzepatide weight regain remains elusive, emerging research has identified several strategies that may reduce the magnitude and rate of post-treatment weight increase. These approaches target the various biological and behavioral mechanisms driving regain.
Gradual Dose Tapering Protocols
Rather than abrupt cessation, some researchers have investigated whether gradually reducing tirzepatide dosage might ease the metabolic transition:
Stepwise Reduction Approach:
- Reduce from maintenance dose (e.g., 15mg) to intermediate dose (10mg) for 4-6 weeks
- Further reduce to lower dose (5mg or 2.5mg) for additional 4-6 weeks
- Monitor weight and metabolic parameters throughout
Preliminary data suggests this approach may reduce the initial rate of regain, though long-term outcomes (12+ months) show similar total regain compared to abrupt discontinuation. The primary benefit appears to be psychological, allowing subjects time to adjust to returning appetite signals.
Transitional Pharmacological Support
Some research protocols have examined whether transitioning to alternative interventions might preserve weight loss:
Maintenance Therapy Options Under Investigation:
- Lower-dose GLP-1 receptor agonists for sustained appetite modulation
- Combination approaches with complementary mechanisms (e.g., metabolic modulators)
- Intermittent dosing schedules (e.g., weekly rather than continuous treatment)
While theoretically promising, long-term efficacy and safety data for these approaches remain limited in 2025, representing an active area of ongoing investigation.
Dietary Interventions for Weight Maintenance
Nutritional strategies play a crucial role in mitigating tirzepatide weight regain. Research-supported approaches include:
High-Protein Dietary Patterns 🥩
Maintaining protein intake at 1.2-1.6 g/kg body weight appears to help preserve lean mass and support satiety during the post-treatment period. Protein’s high thermic effect and satiety-promoting properties provide mechanical advantages against regain.
Structured Meal Timing ⏰
Time-restricted feeding patterns (e.g., 8-10 hour eating windows) have shown promise in some studies for weight maintenance, potentially by optimizing circadian metabolic rhythms and reducing overall caloric intake.
Volumetric Approaches 🥗
Emphasizing low-energy-density foods (vegetables, fruits, lean proteins) helps maintain satiety while controlling caloric intake—particularly important as tirzepatide’s appetite-suppressing effects wane.
Monitoring and Accountability 📱
Regular self-weighing (daily or weekly), food logging, and structured check-ins correlate with better weight maintenance outcomes across multiple studies. These behavioral tools provide early warning of regain trends.
Exercise and Physical Activity Protocols
Physical activity represents another critical component of post-treatment weight maintenance strategies:
Resistance Training 💪
Progressive resistance exercise 2-3 times weekly helps preserve lean muscle mass, which is crucial for maintaining metabolic rate. Studies show subjects who engage in regular strength training experience 15-25% less weight regain compared to sedentary counterparts.
Cardiovascular Exercise 🏃
Moderate-intensity aerobic activity (150-300 minutes weekly) contributes to energy expenditure and metabolic health. Higher volumes (300+ minutes weekly) show stronger associations with weight maintenance.
Non-Exercise Activity Thermogenesis (NEAT) 🚶
Increasing daily movement through lifestyle modifications (standing desks, walking meetings, active transportation) can meaningfully impact total energy expenditure without requiring structured exercise sessions.
Combined Protocols
Research consistently demonstrates that combining resistance and cardiovascular training produces superior outcomes for preventing tirzepatide weight regain compared to either modality alone.
Behavioral and Psychological Interventions
The psychological dimensions of weight maintenance deserve equal attention to physiological strategies:
Cognitive Behavioral Approaches:
- Identifying and modifying eating triggers
- Developing non-food coping mechanisms for stress and emotions
- Building self-efficacy for long-term behavior change
- Restructuring environmental cues that promote overeating
Mindfulness-Based Interventions:
Practices emphasizing present-moment awareness during eating, hunger/satiety recognition, and non-judgmental observation of food thoughts show promise in reducing emotional and impulsive eating patterns that contribute to regain.
Social Support Structures:
Engagement with support groups, accountability partners, or professional coaching correlates with improved weight maintenance. The social reinforcement and shared experience appear to buffer against the isolation often accompanying weight management efforts.
Metabolic Monitoring and Early Intervention
Proactive monitoring allows for early detection and intervention when regain begins:
Key Metrics to Track:
- Body weight (weekly minimum)
- Waist circumference (monthly)
- Fasting glucose and HbA1c (quarterly)
- Lipid panel (semi-annually)
- Blood pressure (weekly to monthly)
Intervention Thresholds:
Establishing predetermined action points (e.g., regain of 2-3% body weight) triggers intensified behavioral interventions before substantial regain occurs. This proactive approach shows better outcomes than reactive responses to large weight increases.
For researchers developing and testing these interventions, access to research-grade peptides enables rigorous investigation of mechanisms and optimization of protocols.
Individual Variability in Tirzepatide Weight Regain: Why Responses Differ
One of the most striking aspects of tirzepatide weight regain research is the substantial heterogeneity in individual responses. While population averages provide useful benchmarks, the range of outcomes spans from complete weight maintenance to rapid return to baseline or beyond. Understanding the sources of this variability represents a critical frontier in metabolic research.
Genetic and Epigenetic Factors
Emerging research has identified several genetic polymorphisms associated with differential weight regain susceptibility:
FTO Gene Variants 🧬
The fat mass and obesity-associated (FTO) gene shows strong associations with obesity risk and weight regain propensity. Subjects carrying certain FTO variants demonstrate 30-40% greater weight regain following interventions, potentially through effects on appetite regulation and energy expenditure.
MC4R Polymorphisms
Melanocortin-4 receptor variants influence hypothalamic appetite circuits. Specific MC4R polymorphisms correlate with both treatment response to GLP-1 receptor agonists and post-treatment weight trajectories.
Epigenetic Modifications
DNA methylation patterns in genes regulating metabolism and appetite show alterations following weight loss that may persist after treatment cessation, potentially “programming” the body for regain. This represents an active area of investigation in 2025.
Baseline Metabolic Phenotype
Pre-treatment metabolic characteristics significantly influence post-treatment outcomes:
Insulin Sensitivity Status 📊
Subjects with preserved insulin sensitivity at baseline demonstrate superior weight maintenance compared to those with significant insulin resistance. The mechanistic basis likely involves more favorable hormonal profiles and metabolic flexibility.
Resting Metabolic Rate
Individuals with higher baseline metabolic rates relative to predicted values show less pronounced metabolic adaptation during weight loss and better maintenance afterward. Those with already-suppressed metabolic rates face compounded challenges.
Adipose Tissue Distribution
Visceral adiposity patterns versus subcutaneous fat distribution influence metabolic health and weight regain trajectories. Higher visceral fat correlates with greater metabolic dysfunction and more challenging maintenance.
Gut Microbiome Composition
The intestinal microbiome has emerged as a significant modulator of weight regulation and tirzepatide weight regain:
Bacterial Diversity:
Higher microbial diversity at baseline and maintenance of diversity during treatment associate with better post-treatment outcomes. Specific bacterial taxa (e.g., Akkermansia muciniphila, Christensenellaceae) show protective correlations.
Metabolite Production:
Gut bacteria produce metabolites (short-chain fatty acids, bile acid derivatives) that influence host metabolism, appetite regulation, and energy harvest from food. Microbiome profiles that favor beneficial metabolite production may confer resistance to regain.
Microbiome Stability:
Subjects whose microbiome composition remains relatively stable during weight loss show better maintenance than those experiencing dramatic shifts, suggesting microbiome resilience as a protective factor.
Behavioral and Psychological Characteristics
Individual differences in behavioral patterns and psychological traits substantially impact outcomes:
Eating Behavior Phenotypes
Emotional Eaters: Those who eat in response to stress or emotions face greater challenges during the post-treatment period when pharmacological appetite suppression wanes
- Restrained Eaters: Individuals with chronic dietary restraint patterns may experience greater vulnerability to disinhibition and regain
- External Eaters: Those highly responsive to environmental food cues show increased susceptibility to obesogenic environments
Self-Regulation Capacity:
Executive function, impulse control, and self-monitoring capabilities predict weight maintenance success. These cognitive capacities enable consistent implementation of maintenance behaviors despite environmental challenges.
Motivation and Goal Orientation:
Intrinsic motivation (internal health values) versus extrinsic motivation (external appearance pressures) differentially predict long-term adherence to maintenance behaviors, with intrinsic motivation showing superior sustainability.
Treatment-Related Variables
Aspects of the treatment experience itself influence subsequent regain:
Dose and Duration Effects:
While mentioned previously, individual responses to different dosing strategies vary considerably. Some subjects achieve excellent outcomes with lower doses and shorter durations, while others require maximum doses and extended treatment.
Adverse Effect Experience:
Subjects who experienced significant gastrointestinal side effects during treatment may have developed aversive associations with eating that dissipate post-treatment, potentially contributing to rebound increases in intake.
Behavioral Engagement During Treatment:
The degree to which subjects actively engaged in lifestyle modifications during pharmacological treatment strongly predicts post-treatment success. Those who relied exclusively on medication without developing sustainable habits face steeper challenges.
Socioeconomic and Environmental Context
External factors beyond individual biology significantly influence tirzepatide weight regain trajectories:
Food Environment Access 🏪
Availability of healthy food options, food costs, and neighborhood walkability affect the feasibility of maintaining weight loss behaviors. Obesogenic environments create constant challenges that require sustained effort to navigate.
Social Networks:
The eating behaviors and body weights of close social contacts influence individual outcomes through both modeling and normative effects. Supportive social networks facilitate maintenance, while unsupportive environments hinder it.
Occupational Demands:
Work schedules, stress levels, and physical activity requirements of employment affect energy balance and behavioral consistency. Shift work and high-stress occupations particularly challenge weight maintenance.
Economic Resources:
Financial capacity to purchase quality foods, access fitness facilities, and obtain professional support services creates disparities in maintenance success across socioeconomic groups.
Understanding this multifaceted variability is essential for researchers developing personalized approaches to preventing tirzepatide weight regain. For those investigating these mechanisms, specialized research compounds provide tools for examining the complex interactions between pharmacological, metabolic, and behavioral factors.
Long-Term Implications and Future Research Directions
As the scientific community accumulates more data on tirzepatide weight regain, several important questions and implications have emerged that will shape future research and clinical approaches to metabolic health.
Metabolic Memory and Long-Term Health Outcomes
Even when significant weight regain occurs, some metabolic improvements may persist:
Residual Metabolic Benefits ✨
Studies tracking subjects 2-3 years post-treatment reveal that even those who regain most lost weight often maintain modest improvements in:
- Glycemic control (HbA1c 0.3-0.5% lower than pre-treatment baseline)
- Lipid profiles (particularly triglycerides)
- Inflammatory markers (though attenuated compared to during treatment)
This “metabolic memory” suggests that even temporary periods of improved metabolic health may confer lasting benefits, though the magnitude and duration of these effects require further investigation.
Cardiovascular Implications:
Long-term cardiovascular outcome data following tirzepatide discontinuation remains limited in 2025. Whether the weight cycling pattern (loss during treatment, regain after cessation) poses cardiovascular risks compared to stable obesity represents an important research question.
Beta Cell Function:
For subjects with impaired glucose tolerance or type 2 diabetes, temporary improvement in glycemic control during treatment may provide “rest” for pancreatic beta cells, potentially preserving function longer-term even after weight regain. This hypothesis requires longitudinal validation.
Optimal Treatment Paradigms
The challenge of tirzepatide weight regain raises fundamental questions about optimal treatment approaches:
Continuous Versus Intermittent Therapy 🔄
Should metabolic peptide interventions be conceptualized as:
- Chronic continuous therapy (similar to blood pressure or cholesterol management)
- Intermittent courses (treatment periods followed by maintenance phases)
- Responsive dosing (adjusting based on weight and metabolic markers)
Each paradigm has different implications for efficacy, safety, cost, and patient burden. Research in 2025 is actively exploring these alternatives.
Combination and Sequential Approaches:
Rather than monotherapy, future protocols may employ:
- Sequential interventions targeting different mechanisms
- Combination therapies with complementary effects
- Integration of pharmacological and non-pharmacological modalities from treatment initiation
Personalized Medicine Applications:
As understanding of genetic, metabolic, and behavioral predictors advances, tailoring treatment approaches to individual phenotypes may optimize outcomes. Precision medicine approaches could identify who benefits from:
- Longer treatment durations
- Higher maintenance doses
- Specific behavioral intervention types
- Alternative or combination pharmacological approaches
Novel Therapeutic Targets
Research into tirzepatide weight regain mechanisms is revealing new potential intervention points:
Metabolic Adaptation Modulators
Compounds that prevent or reverse adaptive thermogenesis could help maintain energy expenditure post-treatment. Targets under investigation include:
- Mitochondrial uncoupling agents
- Brown adipose tissue activators
- Thyroid hormone analogs with metabolic selectivity
Appetite Regulation Beyond GLP-1:
While GLP-1 and GIP represent powerful appetite modulators, other systems offer additional targets:
- Amylin analogs (e.g., cagrilintide)
- Leptin sensitizers
- Ghrelin antagonists
- Neuropeptide Y pathway modulators
Microbiome Interventions:
Targeted modification of gut microbiome composition through:
- Precision probiotics selected for metabolic benefits
- Prebiotic fibers supporting beneficial bacterial populations
- Fecal microbiota transplantation from metabolically healthy donors
Epigenetic Modifiers:
Interventions that alter DNA methylation or histone modifications to reprogram metabolic setpoints represent a frontier area, though practical applications remain distant.
Behavioral Science Integration
Future approaches to preventing tirzepatide weight regain will likely emphasize behavioral science integration:
Digital Health Technologies 📱
- AI-powered coaching applications providing real-time behavioral support
- Wearable devices tracking activity, sleep, and physiological parameters
- Social platforms connecting individuals for peer support
- Gamification strategies enhancing engagement and adherence
Habit Formation Science:
Applying principles from behavioral psychology to build automatic, sustainable behaviors during treatment that persist afterward:
- Implementation intentions (if-then planning)
- Environmental design (choice architecture)
- Habit stacking (linking new behaviors to established routines)
Acceptance and Commitment Approaches:
Rather than fighting biological drives, helping individuals develop psychological flexibility to experience hunger and cravings without automatic behavioral responses may support long-term maintenance.
Research Methodology Advances
Improving understanding of tirzepatide weight regain requires methodological innovations:
Longer Follow-Up Periods:
Most current data extends only 12-24 months post-treatment. Studies tracking subjects 5-10 years will provide crucial information about long-term trajectories and health outcomes.
Mechanistic Studies:
Deep phenotyping approaches examining:
- Continuous glucose monitoring throughout treatment and discontinuation
- Energy expenditure via doubly labeled water or metabolic chambers
- Appetite hormone dynamics with frequent sampling
- Brain imaging studies of reward and appetite circuits
- Muscle and adipose tissue biopsies for molecular analyses
Real-World Evidence:
Complementing controlled trials with observational studies of real-world use patterns, outcomes, and factors influencing success in diverse populations and settings.
For researchers contributing to these advances, access to high-quality research materials remains essential for rigorous, reproducible investigation.
Ethical and Access Considerations
As the field advances, important ethical questions emerge:
Treatment Duration and Dependency:
If optimal outcomes require indefinite treatment, questions arise about:
- Long-term safety with decades of use
- Cost and accessibility implications
- Psychological effects of medication dependency
- Resource allocation in healthcare systems
Weight Cycling Concerns:
Whether repeated cycles of loss and regain pose health risks compared to stable weight (even if elevated) requires careful examination to ensure interventions provide net benefit.
Equity and Access:
Ensuring that advances in metabolic therapeutics benefit diverse populations rather than exacerbating health disparities represents a crucial consideration as the field develops.
Practical Implications for Research Design and Protocol Development
For researchers designing studies involving tirzepatide or similar metabolic peptides, understanding tirzepatide weight regain patterns has important practical implications for protocol development and outcome interpretation.
Study Design Considerations
Follow-Up Duration Planning 📅
Given that substantial regain occurs within 12 months of discontinuation, studies aiming to assess durability of effects should include:
- Minimum 12-month post-treatment follow-up
- Ideally 24-month or longer observation periods
- Frequent assessment points (monthly or quarterly) to capture regain trajectory
Control Group Selection:
Appropriate comparators depend on research questions:
- Placebo controls for mechanistic studies
- Active comparators (other weight loss interventions) for comparative effectiveness
- Usual care controls for pragmatic trials
- Within-subject designs (subjects as their own controls) for regain studies
Outcome Measure Selection:
Beyond simple weight change, comprehensive assessment should include:
- Body composition (lean mass versus fat mass)
- Metabolic parameters (glucose, insulin, lipids)
- Appetite and satiety measures
- Quality of life and psychological outcomes
- Behavioral adherence metrics
Statistical Analysis Approaches
Handling Missing Data:
Weight regain studies often face high attrition as subjects disengage after treatment ends. Appropriate methods include:
- Multiple imputation techniques
- Mixed-effects models that use all available data
- Sensitivity analyses examining different missing data assumptions
- Pattern mixture models when missingness relates to outcomes
Trajectory Modeling:
Rather than simple endpoint comparisons, modeling weight trajectories over time provides richer information:
- Growth curve models capturing individual regain patterns
- Latent class analyses identifying subgroups with distinct trajectories
- Time-to-event analyses for clinically significant regain thresholds
Predictive Modeling:
Machine learning approaches can identify combinations of variables predicting regain:
- Random forests for variable importance
- Gradient boosting for prediction accuracy
- Neural networks for complex non-linear relationships
Sample Size and Power Considerations
Accounting for expected tirzepatide weight regain affects power calculations:
Effect Size Expectations:
If comparing interventions to prevent regain, realistic effect sizes are modest (e.g., 15-25% reduction in regain), requiring larger samples than initial weight loss studies where effects are more dramatic.
Variability Estimates:
High individual variability in regain patterns necessitates larger samples to detect meaningful differences between groups. Standard deviations for weight regain often exceed those during active treatment.
Attrition Planning:
Anticipating 30-50% loss to follow-up in post-treatment phases requires oversizing initial recruitment to maintain adequate power for primary analyses.
Ethical Considerations in Research
Informed Consent Elements:
Subjects should receive clear information about:
- Expected weight regain following treatment discontinuation
- Uncertainty about long-term effects of weight cycling
- Availability (or lack thereof) of proven maintenance strategies
Equipoise and Intervention Selection:
When genuine uncertainty exists about optimal approaches, randomization to different maintenance strategies is ethically appropriate. However, denying proven effective interventions (even if imperfect) raises concerns.
Post-Study Access:
Consideration of whether and how to provide ongoing access to interventions after research participation ends, particularly for subjects who achieved significant health benefits.
Quality Assurance in Peptide Research
For studies utilizing research-grade peptides like tirzepatide, quality assurance is paramount:
Purity and Authentication ✓
- Certificate of analysis verification
- Independent testing when possible
- Proper storage conditions maintained
- Stability monitoring throughout study duration
Standardization Across Sites:
Multi-site studies require:
- Consistent peptide sources and lots
- Standardized reconstitution protocols
- Uniform storage and handling procedures
- Regular quality checks
Researchers can ensure quality by sourcing from established suppliers with documented purity standards and comprehensive product information.
Data Management and Transparency
Comprehensive Data Collection:
Capturing detailed information enables secondary analyses and contributes to broader scientific understanding:
- Baseline demographic and metabolic characteristics
- Treatment adherence and adverse events
- Concurrent interventions and medications
- Behavioral and lifestyle factors
Open Science Practices:
Contributing to cumulative knowledge through:
- Pre-registration of protocols and analysis plans
- Data sharing (with appropriate privacy protections)
- Publication of null and negative findings
- Transparent reporting of all outcomes
Translational Considerations
Bridging Research and Application:
Study designs should consider:
- Feasibility of interventions in real-world settings
- Scalability and cost-effectiveness
- Acceptability to diverse populations
- Implementation barriers and facilitators
Stakeholder Engagement:
Involving patients, clinicians, and other stakeholders in research design ensures relevance and increases likelihood of findings being translated into practice.
Integrating Knowledge: A Systems Perspective on Tirzepatide Weight Regain
Understanding tirzepatide weight regain requires integrating multiple levels of biological organization and environmental context. A systems perspective reveals how molecular, physiological, behavioral, and social factors interact to determine post-treatment outcomes.
The Multi-Level Determinants Framework
Molecular and Cellular Level 🔬
- Receptor expression and signaling cascades
- Adipocyte biology and lipid metabolism
- Mitochondrial function and energy production
- Gene expression and epigenetic modifications
Organ System Level:
- Hypothalamic appetite regulation circuits
- Gastrointestinal hormone secretion
- Pancreatic insulin and glucagon production
- Adipose tissue endocrine function
Whole Organism Level:
- Energy balance and metabolic rate
- Body composition changes
- Hormonal profiles and circadian rhythms
- Physical activity and movement patterns
Behavioral and Psychological Level:
- Eating behaviors and food choices
- Exercise habits and sedentary time
- Stress management and coping strategies
- Self-monitoring and goal-setting
Social and Environmental Level:
- Food availability and accessibility
- Social norms and support networks
- Built environment and activity opportunities
- Economic resources and constraints
Dynamic Interactions and Feedback Loops
These levels don’t operate independently—they interact through complex feedback mechanisms:
Example: The Appetite Regulation Cascade
- Tirzepatide discontinuation → decreased GLP-1 receptor activation (molecular)
- Reduced hypothalamic satiety signaling (organ system)
- Increased hunger and decreased fullness (whole organism)
- Greater food intake and portion sizes (behavioral)
- Food choices influenced by availability and social context (environmental)
- Resulting caloric surplus → weight regain (whole organism)
- Adipose expansion → altered hormone secretion (organ system)
- Changed gene expression in metabolic tissues (molecular)
This cascade illustrates how changes at one level propagate through the system, with each level both influencing and being influenced by others.
Leverage Points for Intervention
A systems perspective reveals multiple potential intervention points:
High-Leverage Interventions (affecting multiple downstream processes):
- Pharmacological approaches maintaining receptor activation
- Environmental redesign reducing obesogenic cues
- Behavioral skills enabling consistent healthy choices despite biological drives
Supporting Interventions (reinforcing high-leverage changes):
- Social support enhancing behavioral adherence
- Metabolic monitoring enabling responsive adjustments
- Stress management reducing emotional eating triggers
System Resilience Factors (buffering against perturbations):
- Metabolic flexibility and insulin sensitivity
- Diverse behavioral repertoire for weight management
- Strong intrinsic motivation and self-efficacy
- Supportive social and physical environments
Individual Variability as System Configuration
The substantial individual differences in tirzepatide weight regain can be understood as different system configurations:
Some individuals possess configurations favoring weight maintenance:
- Preserved metabolic rate and insulin sensitivity
- Strong executive function and self-regulation
- Supportive environments and social networks
- Favorable genetic and epigenetic profiles
Others face configurations promoting regain:
- Metabolic adaptation and insulin resistance
- Impaired executive function or high impulsivity
- Obesogenic environments and limited resources
- Genetic variants affecting appetite and metabolism
Effective interventions must account for these different starting configurations, suggesting the value of personalized approaches tailored to individual system characteristics.
Implications for Research and Practice
This systems perspective suggests several important principles:
Multimodal Interventions: Single-level interventions (e.g., medication alone) face limitations because other system levels continue exerting influence. Combining interventions across levels (pharmacological + behavioral + environmental) may produce synergistic effects.
Timing and Sequencing: When interventions are introduced matters. Behavioral skill-building during active treatment may be more effective than attempting to develop these skills after discontinuation when biological drives are stronger.
Dynamic Adaptation: Static interventions may be insufficient for dynamic systems. Responsive approaches that adjust based on ongoing monitoring may outperform fixed protocols.
Individual Tailoring: Given different system configurations, one-size-fits-all approaches are unlikely to optimize outcomes. Assessment of individual characteristics across multiple levels can guide personalized intervention selection.
For researchers investigating these complex systems, comprehensive research resources enable examination of mechanisms across multiple levels of biological organization.
Advancing Understanding and Improving Outcomes
Tirzepatide weight regain represents one of the most significant challenges in metabolic research—a phenomenon driven by complex interactions between biological, behavioral, and environmental factors. As research in 2025 continues to illuminate the mechanisms underlying post-treatment weight changes, several key insights have emerged:
Core Principles
✅ Weight regain is biologically driven: The body’s compensatory responses to weight loss—including hormonal changes, metabolic adaptation, and altered appetite regulation—create powerful forces favoring weight regain when pharmacological support is removed.
✅ Individual variability is substantial: Genetic, metabolic, behavioral, and environmental factors create dramatically different trajectories across individuals, with some maintaining excellent outcomes while others experience rapid regain.
✅ Multimodal approaches show promise: Combining pharmacological interventions with behavioral, dietary, and exercise strategies during treatment appears to improve post-treatment maintenance compared to medication alone.
✅ Long-term perspective is essential: Sustainable metabolic health requires moving beyond short-term weight loss to comprehensive strategies supporting lifelong weight management.
Actionable Strategies for Researchers
For those investigating metabolic interventions and tirzepatide weight regain:
Design comprehensive protocols that extend well beyond treatment cessation, capturing long-term outcomes and regain patterns with sufficient follow-up duration and assessment frequency.
Examine mechanisms at multiple levels, from molecular signaling to behavioral patterns to environmental influences, recognizing that understanding requires integration across these domains.
Identify predictors and moderators of individual responses to develop personalized approaches that optimize outcomes based on individual characteristics.
Test maintenance interventions rigorously, comparing different strategies for preventing or minimizing regain with appropriate control groups and adequate statistical power.
Contribute to cumulative knowledge through transparent reporting, data sharing, and publication of all findings—positive, negative, and null—to advance the field collectively.
Future Directions
The trajectory of research on tirzepatide weight regain points toward several promising directions:
- Precision medicine approaches leveraging genetic, metabolic, and behavioral profiling to match individuals with optimal intervention strategies
- Novel therapeutic targets addressing metabolic adaptation, appetite regulation beyond GLP-1, and microbiome modulation
- Digital health integration providing continuous support, monitoring, and adaptive interventions through technology platforms
- Long-term outcome studies tracking health implications over decades rather than months or years
Taking the Next Step
For researchers seeking to contribute to this important area of investigation, ensuring access to high-quality research materials is fundamental. PEPTIDE PRO provides research-grade peptides with documented purity, proper storage conditions, and comprehensive product information—essential foundations for rigorous, reproducible research.
Whether investigating mechanisms of weight regain, testing prevention strategies, or exploring novel therapeutic approaches, the quality and consistency of research materials directly impact the validity and reliability of findings. By maintaining strict quality standards and supporting the research community with fast delivery and professional service, PEPTIDE PRO enables scientists to focus on advancing knowledge rather than questioning material quality.
The challenge of tirzepatide weight regain remains substantial, but continued rigorous investigation is progressively revealing its mechanisms and identifying strategies to improve long-term outcomes. As the scientific community builds on current knowledge, the prospects for developing more effective, sustainable approaches to metabolic health continue to strengthen.